

Does Structured Exercise Improve Cognitive Impairment in People with Mild to Moderate Dementia? A Cost-Effectiveness Analysis from a Confirmatory Randomised Controlled Trial: The Dementia and Physical Activity (DAPA) Trial
- PMID: 30206826
- PMCID: PMC6533370
- DOI: 10.1007/s41669-018-0097-9
Does Structured Exercise Improve Cognitive Impairment in People with Mild to Moderate Dementia? A Cost-Effectiveness Analysis from a Confirmatory Randomised Controlled Trial: The Dementia and Physical Activity (DAPA) Trial
Abstract
Background: Previous studies suggest that physical exercise could slow dementia progression. However, evidence for the cost effectiveness of structured exercise is conflicting and based on small trials.
Objectives: The objective of this study was to compare the cost effectiveness of a tailored, structured, moderate- to high-intensity exercise programme versus usual care in people with mild to moderate dementia.
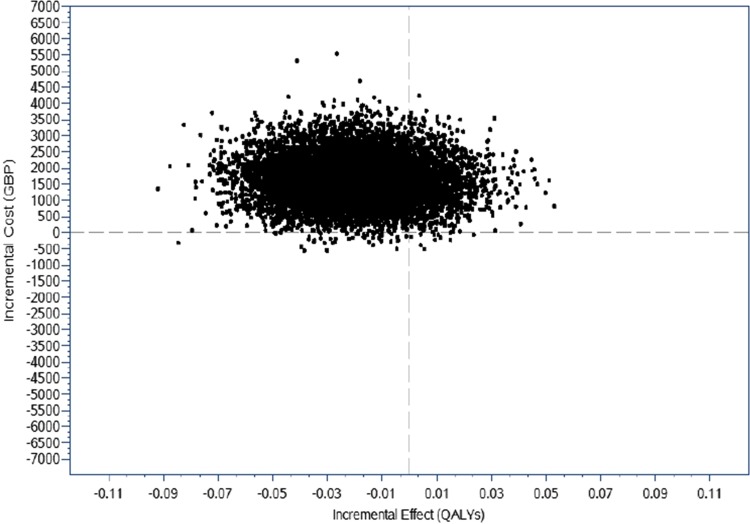
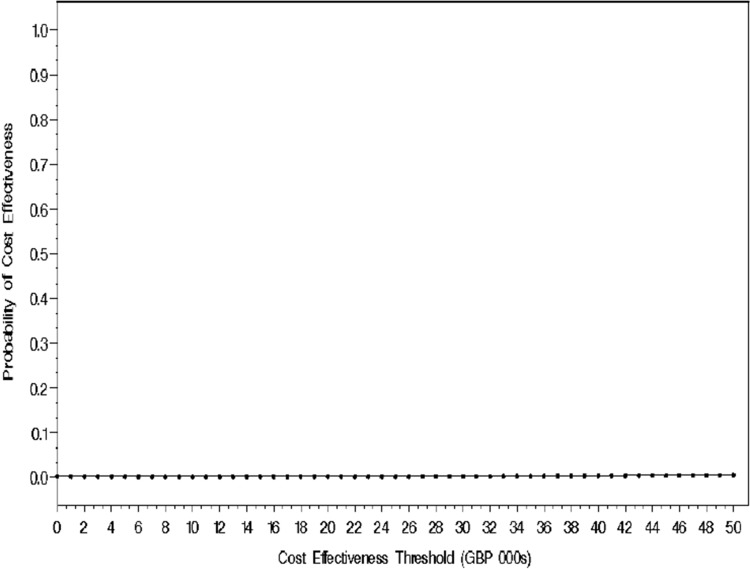
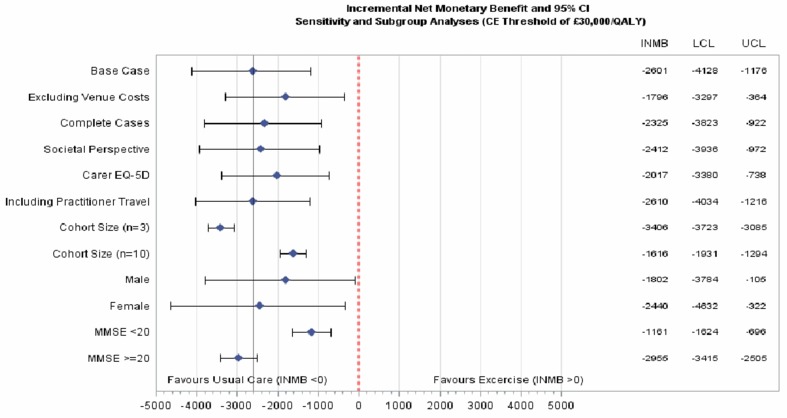
Methods: An economic evaluation was conducted from the UK National Health Service and personal social services perspective, based on data from a large randomised controlled trial. The primary clinical outcome was the participant reported ADAS-Cog (Alzheimer's Disease Assessment Scale-Cognitive Subscale) at 12 months. Costs (£; 2014-2015 prices) were collected prospectively over a 12-month follow-up period. A bivariate regression of costs and quality-adjusted life-years (QALYs), with multiple imputation of missing data, was conducted with the view to estimating the incremental cost per QALY gained and the incremental net monetary benefit (INMB) associated with the exercise programme plus usual care versus usual care. Sensitivity analyses were undertaken to assess the impact of uncertainty surrounding aspects of the economic evaluation, and pre-specified subgroup analyses explored heterogeneity in the cost-effectiveness results.
Results: Participants (n = 494) were randomised to exercise plus usual care or usual care only. By 12 months the mean ADAS-Cog score had worsened slightly to 25.2 (standard deviation [SD] 12.3) in the exercise arm and 23.8 (SD 10.4) in the usual care: difference - 1.4, 95% confidence interval (CI) - 2.6 to - 0.2 (p = 0.03). The mean (standard error [SE]) costs over 12 months for experimental versus control was £5945 (US$7856) versus £4597 (US$6574), respectively; (difference: £1347 [$1926]; p = 0.0426). Mean (SE) QALY estimates were 0.787 (0.012) versus 0.826 (0.019), respectively (p = 0.090). The probability that the exercise programme is cost effective was < 1% across cost-effectiveness thresholds. INMBs ranged between -£2601 (US$3719) and £2158 (US$3086) at cost-effectiveness thresholds between £15,000 (US$21,450) and £30,000 (US$42,900) per QALY. The cost-effectiveness results remained robust to several sensitivity and subgroup analyses.
Conclusions: Building on the clinical results of the trial, which showed that the structured exercise programme evaluated does not slow cognitive impairment in people with mild to moderate dementia, this economic evaluation shows that the programme is not cost effective.
Conflict of interest statement
Dr Iftekhar Khan, Prof. Stavros Petrou, Mr Kamran Khan, Dr Dipesh Mistry, Dr Ranjit Lall, Dr Bart Sheehan and Prof. Sarah Lamb declare no conflicts of interest related to this study.
Figures
References
-
- Matthews FE, Arthur A, Barnes LE, Bond J, Jagger C, Robinson L, et al. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II. Lancet. 2013;382(9902):1405–1412. doi: 10.1016/S0140-6736(13)61570-6. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
