

The respiratory physiome: Clustering based on a comprehensive lung function assessment in patients with COPD
- PMID: 30208035
- PMCID: PMC6135389
- DOI: 10.1371/journal.pone.0201593
The respiratory physiome: Clustering based on a comprehensive lung function assessment in patients with COPD
Abstract
Background: While spirometry and particularly airflow limitation is still considered as an important tool in therapeutic decision making, it poorly reflects the heterogeneity of respiratory impairment in chronic obstructive pulmonary disease (COPD). The aims of this study were to identify pathophysiological clusters in COPD based on an integrated set of standard lung function attributes and to investigate whether these clusters can predict patient-related outcomes and differ in clinical characteristics.
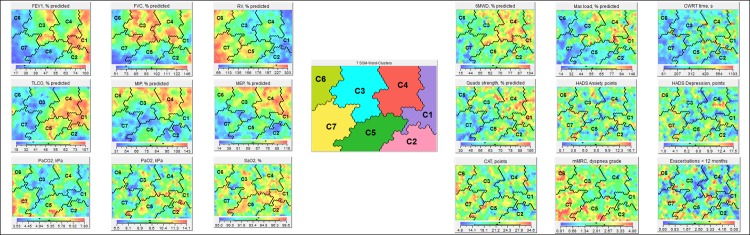
Methods: Clinically stable COPD patients referred for pulmonary rehabilitation underwent an integrated assessment including clinical characteristics, dyspnea score, exercise performance, mood and health status, and lung function measurements (post-bronchodilator spirometry, body plethysmography, diffusing capacity, mouth pressures and arterial blood gases). Self-organizing maps were used to generate lung function based clusters.
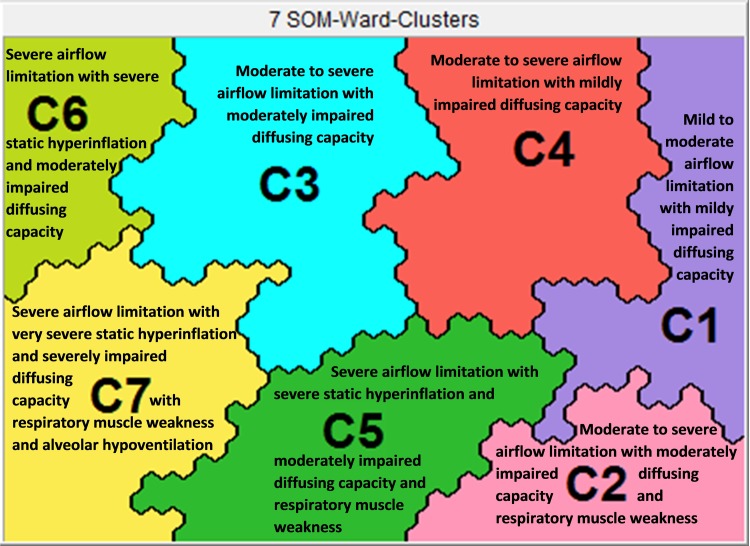
Results: Clustering of lung function attributes of 518 patients with mild to very severe COPD identified seven different lung function clusters. Cluster 1 includes patients with better lung function attributes compared to the other clusters. Airflow limitation is attenuated in clusters 1 to 4 but more pronounced in clusters 5 to 7. Static hyperinflation is more dominant in clusters 5 to 7. A different pattern occurs for carbon monoxide diffusing capacity, mouth pressures and for arterial blood gases. Related to the different lung function profiles, clusters 1 and 4 demonstrate the best functional performance and health status while this is worst for clusters 6 and 7. All clusters show differences in dyspnea score, proportion of men/women, age, number of exacerbations and hospitalizations, proportion of patients using long-term oxygen and number of comorbidities.
Conclusion: Based on an integrated assessment of lung function variables, seven pathophysiological clusters can be identified in COPD patients. These clusters poorly predict functional performance and health status.
Conflict of interest statement
Pharmaceutical company GlaxoSmithKline helped support the CHANCE study (SCO115406). This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no patents, products in development or marketed products to declare.
Figures
References
-
- Wedzicha J.A., et al. , Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med, 2013. 1(3): p. 199–209. 10.1016/S2213-2600(13)70052-3 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
