

Predictive value of a diagnostic block in focal nerve injury with neuropathic pain when surgery is considered
- PMID: 30208078
- PMCID: PMC6135496
- DOI: 10.1371/journal.pone.0203345
Predictive value of a diagnostic block in focal nerve injury with neuropathic pain when surgery is considered
Abstract
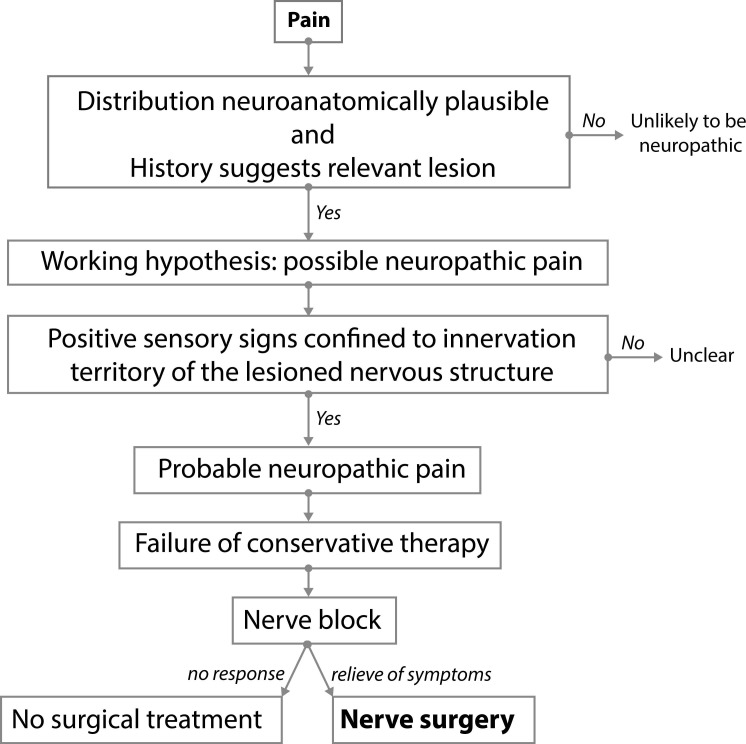
Object: In patients with focal nerve injury and neuropathic pain cutting the nerve to obtain permanent pain reduction can be considered. Surgery is indicated only if a diagnostic nerve block provides temporary pain relief. We evaluated the predictive value of a block on the outcome of surgery.
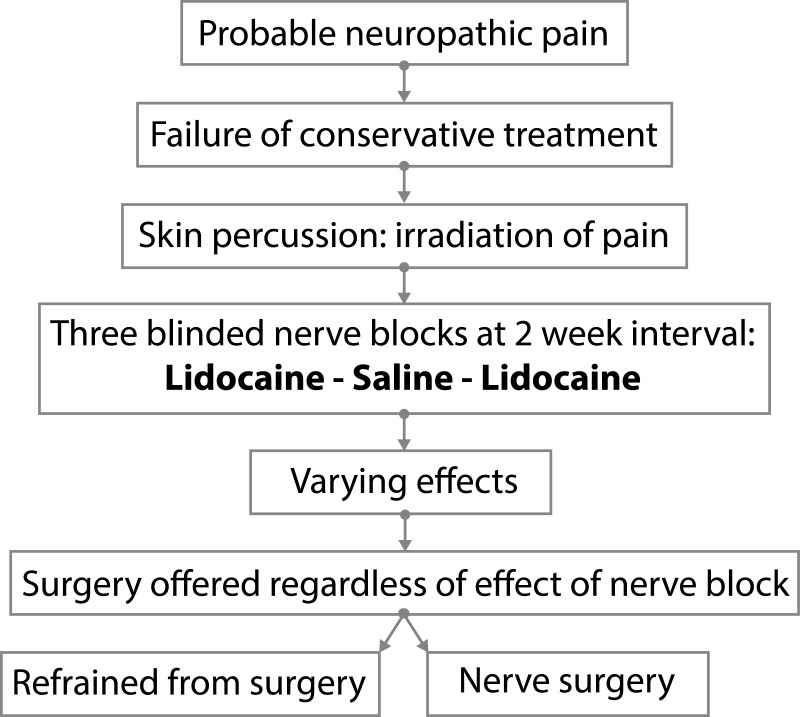
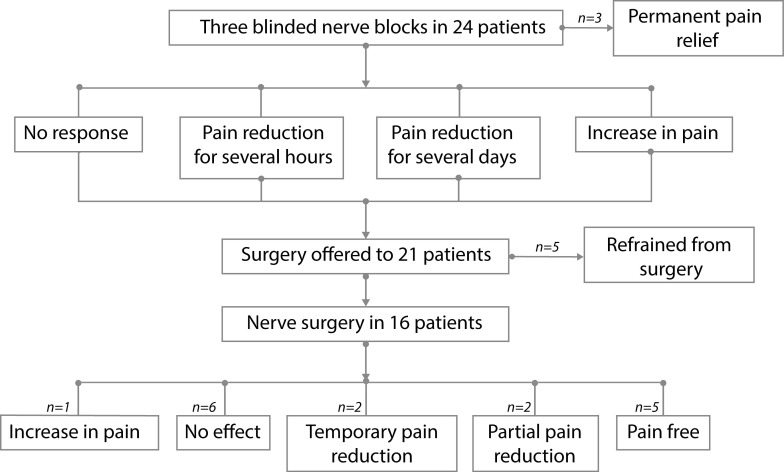
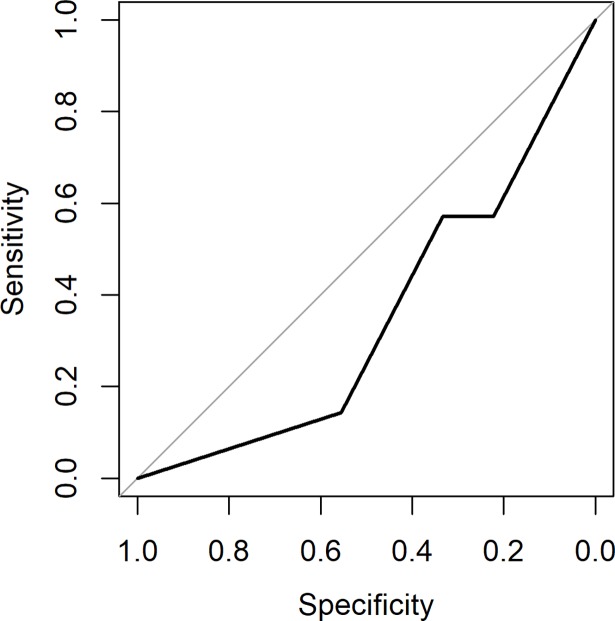
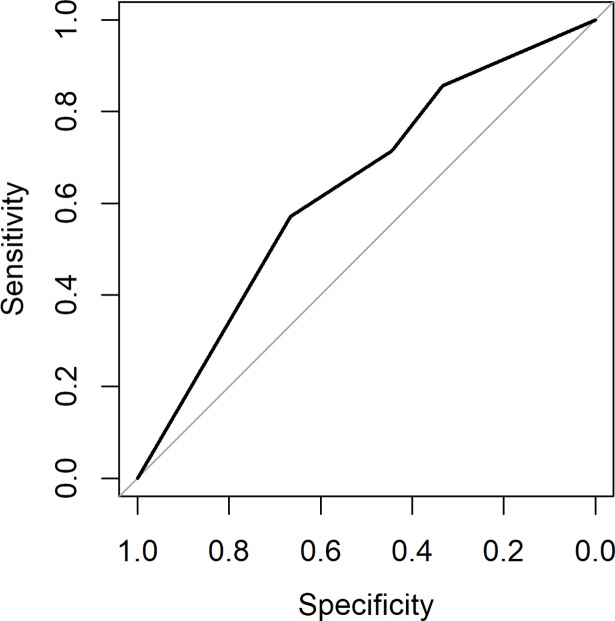
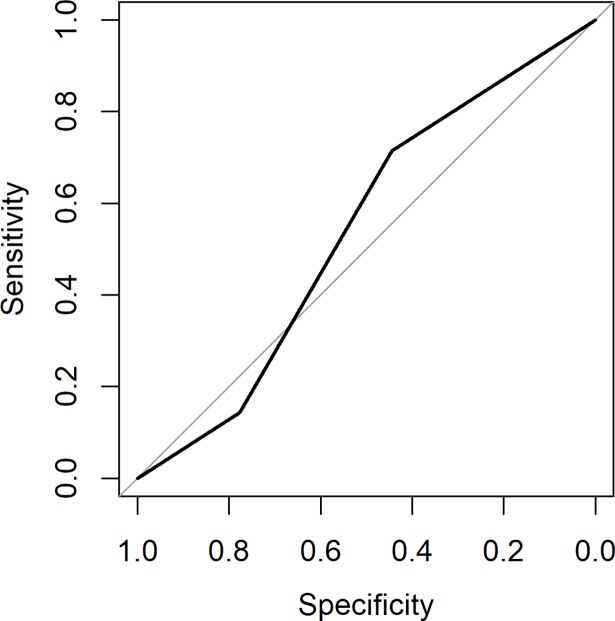
Methods: In total, three blocks were performed at two week intervals. Patients were blinded to injections containing lidocaine 1% and a placebo was included. Surgery was offered regardless of the effect of the blocks. Twenty-four patients received 72 blocks. Sixteen patients opted for surgery, 5 patients refrained from surgery, and in 3 the blocks provided permanent pain relief. The predictive ability of the block on the outcome of surgery was assessed by calculating the area under a Receiver Operating Characteristic curve (AUC).
Results: The AUC of the first lidocaine block was 0.35 with a 95% confidence interval from 0.077 to 0.62. At 95% confidence (two-sided), the AUC is less than 0.62, and hence the predictive ability of the block was poor. The outcome of the second lidocaine block and saline block did not change the conclusion of the first block.
Conclusions: We conclude that the use of blocks to select patients for surgery should be critically appraised.
Perspective: A pain relieving response to one open block is currently considered mandatory before patients with focal nerve injury and neuropathic pain are offered surgery. Blinded blocks including a placebo show that responses for selection should be carefully interpreted because they may not be as predictive as generally presumed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Attal N, Bouhassira D. Pharmacotherapy of neuropathic pain: which drugs, which treatment algorithms? Pain 2015. April;156 Suppl 1:S104–S114. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
