

The Latent Structure of Negative Symptoms in Schizophrenia
- PMID: 30208377
- PMCID: PMC6583036
- DOI: 10.1001/jamapsychiatry.2018.2475
The Latent Structure of Negative Symptoms in Schizophrenia
Abstract
Importance: Negative symptoms are associated with a range of poor clinical outcomes, and currently available treatments generally do not produce a clinically meaningful response. Limited treatment progress may be owing in part to poor clarity regarding latent structure. Prior studies have inferred latent structure using exploratory factor analysis, which has led to the conclusion that there are 2 dimensions reflecting motivation and pleasure (MAP) and diminished expressivity (EXP) factors. However, whether these conclusions are statistically justified remains unclear because exploratory factor analysis does not test latent structure. Confirmatory factor analysis (CFA) is needed to test competing models regarding the latent structure of a construct.
Objective: To evaluate the fit of 4 models of the latent structure of negative symptoms in schizophrenia using CFA.
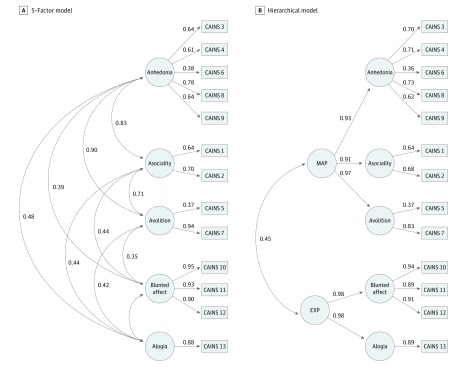
Design, setting, and participants: Three cross-sectional studies were conducted on outpatients with schizophrenia who were rated on the 3 most conceptually contemporary measures: Scale for the Assessment of Negative Symptoms (SANS), Brief Negative Symptom Scale (BNSS), and Clinical Assessment Interview for Negative Symptoms (CAINS). Confirmatory factor analysis evaluated the following 4 models: (1) a 1-factor model; (2) a 2-factor model with EXP and MAP factors; (3) a 5-factor model with separate factors for the 5 domains of the National Institute of Mental Health consensus development conference (blunted affect, alogia, anhedonia, avolition, and asociality); and (4) a hierarchical model with 2 second-order factors reflecting EXP and MAP and 5 first-order factors reflecting the 5 consensus domains.
Main outcomes and measures: Outcomes included CFA model fit statistics derived from symptom severity scores on the SANS, BNSS, and CAINS.
Results: The study population included 860 outpatients with schizophrenia (68.0% male; mean [SD] age, 43.0 [11.4] years). Confirmatory factor analysis was conducted on each scale, including 268 patients for the SANS, 192 for the BNSS, and 400 for the CAINS. The 1- and 2-factor models provided poor fit for the SANS, BNSS, and CAINS as indicated by comparative fit indexes (CFIs) and Tucker Lewis indexes (TLIs) less than 0.950, RMSEAs that exceeded the 0.080 threshold, and WRMRs greater than 1.00. The 5-factor and hierarchical models provided excellent fit, with the 5-factor model being more parsimonious. The CFIs and TLIs met the 0.95 threshold and the 1.00 threshold for both factor models with all 3 measures. Interestingly, the RMSEAs for the 5-factor model and the hierarchical model fell under the 0.08 threshold for the BNSS and the CAINS but not the SANS.
Conclusions and relevance: These findings suggest that the recent trend toward conceptualizing the latent structure of negative symptoms as 2 distinct dimensions does not adequately capture the complexity of the construct. The latent structure of negative symptoms is best conceptualized in relation to the 5 consensus domains. Implications for identifying pathophysiological mechanisms and targeted treatments are discussed.
Conflict of interest statement
Figures


Similar articles
-
Network Analysis Reveals the Latent Structure of Negative Symptoms in Schizophrenia.Schizophr Bull. 2019 Sep 11;45(5):1033-1041. doi: 10.1093/schbul/sby133. Schizophr Bull. 2019. PMID: 30256991 Free PMC article.
-
Cross-cultural Validation of the 5-Factor Structure of Negative Symptoms in Schizophrenia.Schizophr Bull. 2019 Mar 7;45(2):305-314. doi: 10.1093/schbul/sby050. Schizophr Bull. 2019. PMID: 29912473 Free PMC article.
-
Revisiting the latent structure of negative symptoms in schizophrenia: Evidence from two second-generation clinical assessments.Schizophr Res. 2022 Oct;248:131-139. doi: 10.1016/j.schres.2022.08.016. Epub 2022 Aug 29. Schizophr Res. 2022. PMID: 36037646
-
Meta-analysis of the factor structure of the Scale for the Assessment of Negative Symptoms (SANS) and the Scale for the Assessment of Positive Symptoms (SAPS).Schizophr Res. 2024 Dec;274:464-472. doi: 10.1016/j.schres.2024.10.027. Epub 2024 Nov 7. Schizophr Res. 2024. PMID: 39515256 Review.
-
The brief negative symptom scale in translation: A review of psychometric properties and beyond.Eur Neuropsychopharmacol. 2020 Apr;33:36-44. doi: 10.1016/j.euroneuro.2020.01.018. Epub 2020 Feb 18. Eur Neuropsychopharmacol. 2020. PMID: 32081498 Review.
Cited by
-
Using the big data approach to clarify the structure of restricted and repetitive behaviors across the most commonly used autism spectrum disorder measures.Mol Autism. 2021 May 27;12(1):39. doi: 10.1186/s13229-021-00419-9. Mol Autism. 2021. PMID: 34044873 Free PMC article.
-
Geolocation as a Digital Phenotyping Measure of Negative Symptoms and Functional Outcome.Schizophr Bull. 2020 Dec 1;46(6):1596-1607. doi: 10.1093/schbul/sbaa121. Schizophr Bull. 2020. PMID: 32851401 Free PMC article.
-
Differential improvement of negative-symptom subfactors after cognitive remediation in low-functioning individuals with schizophrenia.Schizophr Res Cogn. 2019 Apr 17;19:100145. doi: 10.1016/j.scog.2019.100145. eCollection 2020 Mar. Schizophr Res Cogn. 2019. PMID: 31828020 Free PMC article.
-
Mapping the Research Domain Criteria Social Processes Constructs to the Social Responsiveness Scale.J Am Acad Child Adolesc Psychiatry. 2020 Nov;59(11):1252-1263.e3. doi: 10.1016/j.jaac.2019.07.938. Epub 2019 Aug 1. J Am Acad Child Adolesc Psychiatry. 2020. PMID: 31376500 Free PMC article.
-
ENIGMA + COINSTAC: Improving Findability, Accessibility, Interoperability, and Re-usability.Neuroinformatics. 2022 Jan;20(1):261-275. doi: 10.1007/s12021-021-09559-y. Epub 2021 Nov 30. Neuroinformatics. 2022. PMID: 34846691 Free PMC article.
References
-
- Bleuler E. Dementia praecox or the group of schizophrenias [in Spanish]. Vertex. 2010;21(93):394-400. - PubMed
-
- Kraepelin E, Robertson MR, eds. Dementia Praecox and Paraphrenia. New York, NY: Krieger Publishing; 1919.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
