

Antiepileptic drug treatment after an unprovoked first seizure: A decision analysis
- PMID: 30209239
- PMCID: PMC6177278
- DOI: 10.1212/WNL.0000000000006319
Antiepileptic drug treatment after an unprovoked first seizure: A decision analysis
Abstract
Objective: To compare the expected quality-adjusted life-years (QALYs) in adult patients undergoing immediate vs deferred antiepileptic drug (AED) treatment after a first unprovoked seizure.
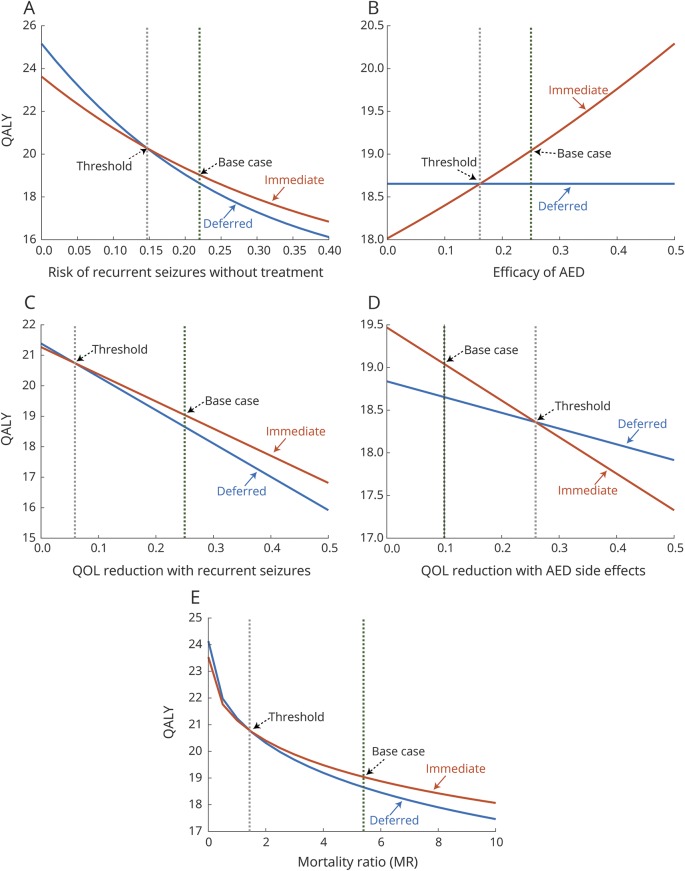
Methods: We constructed a simulated clinical trial (Markov decision model) to compare immediate vs deferred AED treatment after a first unprovoked seizure in adults. Three base cases were considered, representing patients with varying degrees of seizure recurrence risk and effect of seizures on quality of life (QOL). Cohort simulation was performed to determine which treatment strategy would maximize the patient's expected QALYs. Sensitivity analyses were guided by clinical data to define decision thresholds across plausible measurement ranges, including seizure recurrence rate, effect of seizure recurrence on QOL, and efficacy of AEDs.
Results: For patients with a moderate risk of recurrent seizures (52.0% over 10 years after first seizure), immediate AED treatment maximized QALYs compared to deferred treatment. Sensitivity analyses showed that for the preferred choice to change to deferred AED treatment, key clinical measures needed to reach implausible values were 10-year seizure recurrence rate ≤38.0%, QOL reduction with recurrent seizures ≤0.06, and efficacy of AEDs on lowering seizure recurrence rate ≤16.3%.
Conclusion: Our model determined that immediate AED treatment is preferable to deferred treatment in adult first-seizure patients over a wide and clinically relevant range of variables. Furthermore, our analysis suggests that the 10-year seizure recurrence rate that justifies AED treatment (38.0%) is substantially lower than the 60% threshold used in the current definition of epilepsy.
© 2018 American Academy of Neurology.
Figures



Comment in
-
Immediate vs delayed treatment of first unprovoked seizure: To treat, or not to treat?Neurology. 2018 Oct 9;91(15):684-685. doi: 10.1212/WNL.0000000000006304. Epub 2018 Sep 12. Neurology. 2018. PMID: 30209237 No abstract available.
References
-
- Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 2014;55:475–482. - PubMed
-
- Marson A, Jacoby A, Johnson A, et al. Immediate versus deferred antiepileptic drug treatment for early epilepsy and single seizures: a randomised controlled trial. Lancet 2005;365:2007–2013. - PubMed
-
- Randomized clinical trial on the efficacy of antiepileptic drugs in reducing the risk of relapse after a first unprovoked tonic-clonic seizure: First Seizure Trial Group (FIRST Group). Neurology 1993;43:478–483. - PubMed
-
- Musicco M, Beghi E, Solari A, Viani F. Treatment of first tonic-clonic seizure does not improve the prognosis of epilepsy: First Seizure Trial Group (FIRST Group). Neurology 1997;49:991–998. - PubMed
-
- Leone MA, Solari A, Beghi E. Treatment of the first tonic-clonic seizure does not affect long-term remission of epilepsy. Neurology 2006;67:2227–2229. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical