

Clinical prediction of thrombectomy eligibility: A systematic review and 4-item decision tree
- PMID: 30209989
- PMCID: PMC6710617
- DOI: 10.1177/1747493018801225
Clinical prediction of thrombectomy eligibility: A systematic review and 4-item decision tree
Abstract
Background: A clinical large anterior vessel occlusion (LAVO)-prediction scale could reduce treatment delays by allocating intra-arterial thrombectomy (IAT)-eligible patients directly to a comprehensive stroke center.
Aim: To subtract, validate and compare existing LAVO-prediction scales, and develop a straightforward decision support tool to assess IAT-eligibility.
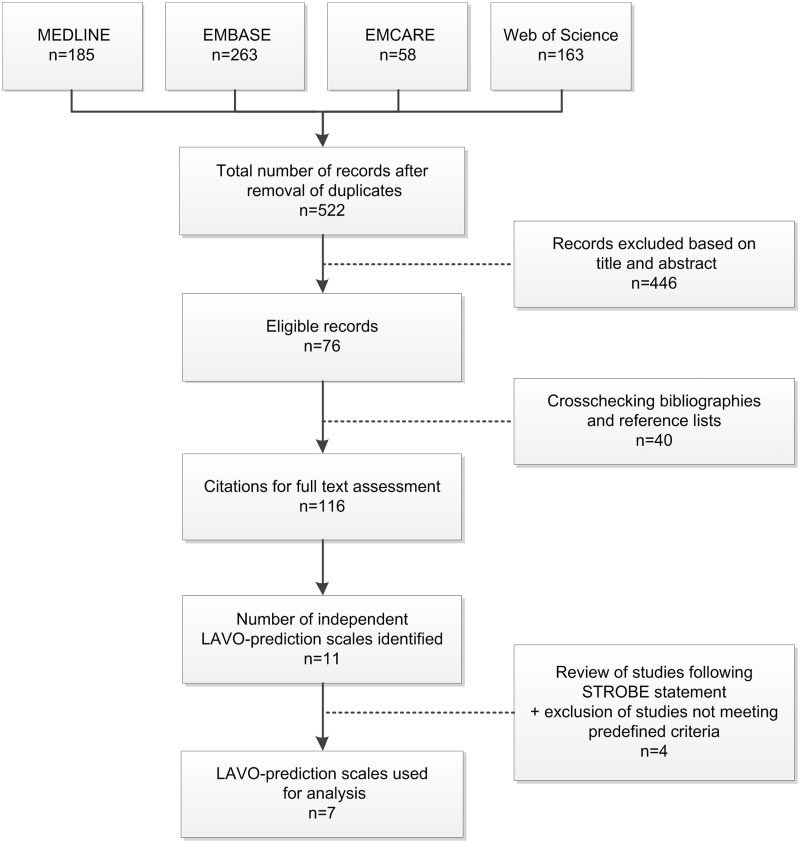
Methods: We performed a systematic literature search to identify LAVO-prediction scales. Performance was compared in a prospective, multicenter validation cohort of the Dutch acute Stroke study (DUST) by calculating area under the receiver operating curves (AUROC). With group lasso regression analysis, we constructed a prediction model, incorporating patient characteristics next to National Institutes of Health Stroke Scale (NIHSS) items. Finally, we developed a decision tree algorithm based on dichotomized NIHSS items.
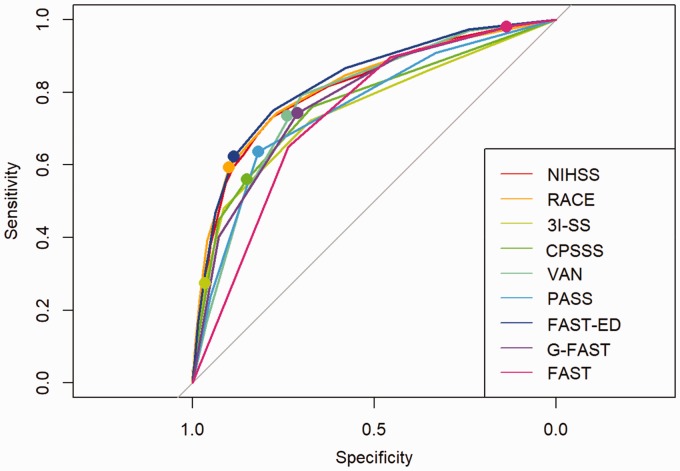
Results: We identified seven LAVO-prediction scales. From DUST, 1316 patients (35.8% LAVO-rate) from 14 centers were available for validation. FAST-ED and RACE had the highest AUROC (both >0.81, p < 0.01 for comparison with other scales). Group lasso analysis revealed a LAVO-prediction model containing seven NIHSS items (AUROC 0.84). With the GACE (Gaze, facial Asymmetry, level of Consciousness, Extinction/inattention) decision tree, LAVO is predicted (AUROC 0.76) for 61% of patients with assessment of only two dichotomized NIHSS items, and for all patients with four items.
Conclusion: External validation of seven LAVO-prediction scales showed AUROCs between 0.75 and 0.83. Most scales, however, appear too complex for Emergency Medical Services use with prehospital validation generally lacking. GACE is the first LAVO-prediction scale using a simple decision tree as such increasing feasibility, while maintaining high accuracy. Prehospital prospective validation is planned.
Keywords: Acute ischemic stroke; clinical scale; endovascular thrombectomy; intra-arterial thrombectomy; large vessel occlusion; prehospital.
Figures

References
-
- Fransen PS, Berkhemer OA, Lingsma HF, et al. Time to reperfusion and treatment effect for acute ischemic stroke: a randomized clinical trial. JAMA Neurol 2016; 73: 190–196. - PubMed
-
- Goyal M, Jadhav AP, Bonafe A, et al. Analysis of Workflow and time to treatment and the effects on outcome in endovascular treatment of acute ischemic stroke: results from the SWIFT PRIME randomized controlled trial. Radiology 2016; 279: 888–897. - PubMed
-
- Meretoja A, Keshtkaran M, Tatlisumak T, Donnan GA, Churilov L. Endovascular therapy for ischemic stroke: save a minute-save a week. Neurology 2017; 88: 2123–2127. - PubMed
-
- Prabhakaran S, Ward E, John S, et al. Transfer delay is a major factor limiting the use of intra-arterial treatment in acute ischemic stroke. Stroke 2011; 42: 1626–1630. - PubMed
-
- Jauch EC, Saver JL, Adams HP, Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013; 44: 870–947. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
