

Gene therapy for hemophilia: what does the future hold?
- PMID: 30210756
- PMCID: PMC6130099
- DOI: 10.1177/2040620718791933
Gene therapy for hemophilia: what does the future hold?
Abstract
Recent phase I/II adeno-associated viral vector-mediated gene therapy clinical trials have reported remarkable success in ameliorating disease phenotype in hemophilia A and B. These trials, which highlight the challenges overcome through decades of preclinical and first in human clinical studies, have generated considerable excitement for patients and caregivers alike. Optimization of vector and transgene expression has significantly improved the ability to achieve therapeutic factor levels in these subjects. Long-term follow-up studies will guide standardization of the approach with respect to the combination of serotype, promoter, dose, and manufacturing processes and inform safety for inclusion of young patients. Certain limitations preclude universal applicability of gene therapy, including transient liver transaminase elevations due to the immune responses to vector capsids or as yet undefined mechanisms, underlying liver disease from iatrogenic viral hepatitis, and neutralizing antibodies to clotting factors. Integrating vectors show promising preclinical results, but manufacturing and safety concerns still remain. The prospect of gene editing for correction of the underlying mutation is on the horizon with considerable potential. Herein, we review the advances and limitations that have resulted in these recent successful clinical trials and outline avenues that will allow for broader applicability of gene therapy.
Keywords: adeno-associated virus; gene therapy; hemophilia; lentivirus.
Conflict of interest statement
Conflict of interest statement: The authors declare that they have no conflicts of interest.
Figures

 ), factor activity
(
), factor activity
( )
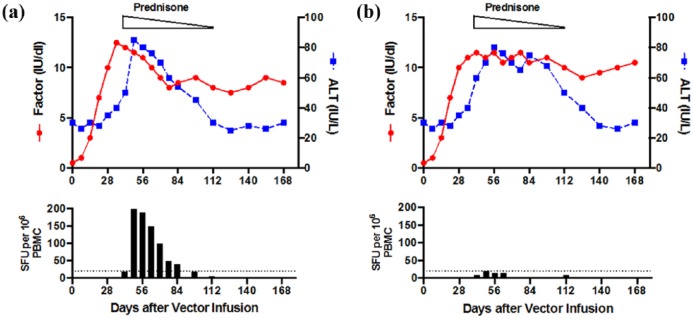
and T-cell enzyme-linked immunospot (ELISPOT). (a) The observation of a
rise in liver alanine aminotransferase (ALT) with coincident decline in
transgene expression is thought to be associated with a cellular immune
response against the AAV capsid as confirmed by positive ELISPOT (bottom
panel). This effect can be rescued with a short course of
corticosteroids (prednisone). (b) In two recent trials, a rise in ALT
does not always correlate with loss of factor activity or positive
T-cell ELISPOT. Although steroids are used in these trials, ALT response
is not uniform in all cases. PBMC, peripheral blood mononuclear cells;
SFU, spot-forming units
)
and T-cell enzyme-linked immunospot (ELISPOT). (a) The observation of a
rise in liver alanine aminotransferase (ALT) with coincident decline in
transgene expression is thought to be associated with a cellular immune
response against the AAV capsid as confirmed by positive ELISPOT (bottom
panel). This effect can be rescued with a short course of
corticosteroids (prednisone). (b) In two recent trials, a rise in ALT
does not always correlate with loss of factor activity or positive
T-cell ELISPOT. Although steroids are used in these trials, ALT response
is not uniform in all cases. PBMC, peripheral blood mononuclear cells;
SFU, spot-forming unitsReferences
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
