

Treatment of Fractures of the Thoracolumbar Spine: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU)
- PMID: 30210959
- PMCID: PMC6130107
- DOI: 10.1177/2192568218771668
Treatment of Fractures of the Thoracolumbar Spine: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU)
Abstract
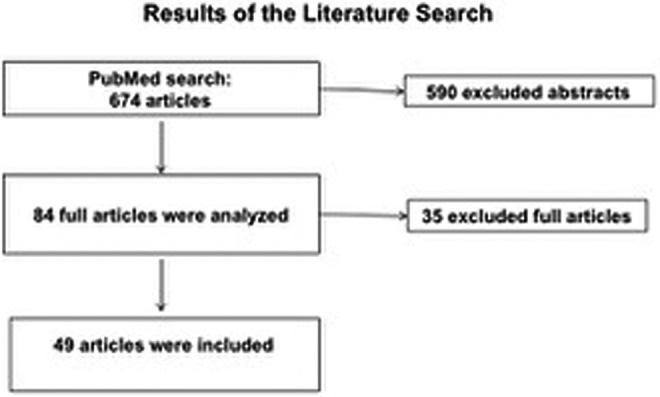
Study design: consensus paper with systematic literature review.
Objective: The aim of this study was to establish recommendations for treatment of thoracolumbar spine fractures based on systematic review of current literature and consensus of several spine surgery experts.
Methods: The project was initiated in September 2008 and published in Germany in 2011. It was redone in 2017 based on systematic literature review, including new AOSpine classification. Members of the expert group were recruited from all over Germany working in hospitals of all levels of care. In total, the consensus process included 9 meetings and 20 hours of video conferences.
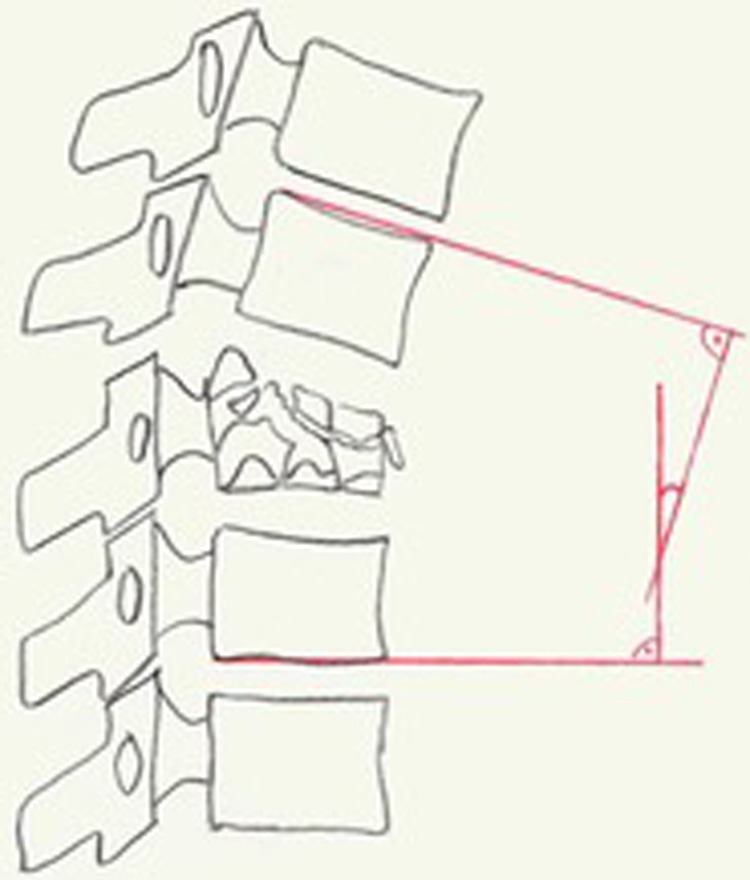
Results: As regards existing studies with highest level of evidence, a clear recommendation regarding treatment (operative vs conservative) or regarding type of surgery (posterior vs anterior vs combined anterior-posterior) cannot be given. Treatment has to be indicated individually based on clinical presentation, general condition of the patient, and radiological parameters. The following specific parameters have to be regarded and are proposed as morphological modifiers in addition to AOSpine classification: sagittal and coronal alignment of spine, degree of vertebral body destruction, stenosis of spinal canal, and intervertebral disc lesion. Meanwhile, the recommendations are used as standard algorithm in many German spine clinics and trauma centers.
Conclusion: Clinical presentation and general condition of the patient are basic requirements for decision making. Additionally, treatment recommendations offer the physician a standardized, reproducible, and in Germany commonly accepted algorithm based on AOSpine classification and 4 morphological modifiers.
Keywords: conservative therapy; morphological modifiers; operative therapy; therapy recommendations; thoracolumbar spine fracture; traumatic vertebral body fractures.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





References
-
- Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003;85-A:773–781. - PubMed
-
- Siebenga J, Leferink VJ, Segers MJ, et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine (Phila Pa 1976). 2006;31:2881–2890. - PubMed
-
- Verheyden AP, Hölzl A, Ekkerlein H, et al. Recommendations for the treatment of thoracolumbar and lumbar spine injuries [in German]. Unfallchirurg. 2011;114:9–16. doi:10.1007/s00113-010-1934-1. - PubMed
-
- Wood KB, Buttermann GR, Phukan R, et al. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: a prospective randomized study with follow-up at sixteen to twenty-two years. J Bone Joint Surg Am. 2015;97:3–9. doi:10.2106/JBJS.N.00226. - PubMed
-
- Scholz M, Kandziora F, Tschauder T, Kremer M, Pingel A. Prospective randomized controlled comparison of posterior vs. posterior-anterior stabilization of thoracolumbar incomplete cranial burst fractures in neurological intact patients: the RASPUTHINE pilot study [published online October 25, 2017]. Eur Spine J. doi:10.1007/s00586-017-5356-4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
