

Spine Fractures in Ankylosing Diseases: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU)
- PMID: 30210963
- PMCID: PMC6130102
- DOI: 10.1177/2192568217736268
Spine Fractures in Ankylosing Diseases: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU)
Abstract
Study design: Review of literature and case series.
Objectives: Update and review of current treatment concepts for spine fractures in patients with ankylosing spinal disorders.
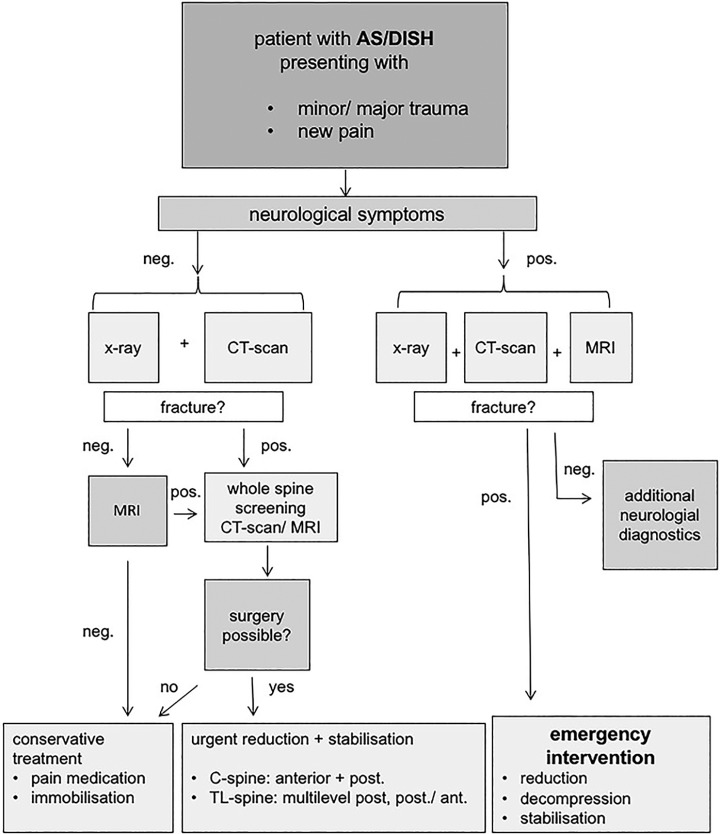
Methods: Case presentation and description of a diagnostic and therapeutic algorithm for unstable spinal injuries with an underlying ankylosing spinal disorder (ASD) of the cervical and thoracolumbar spine.
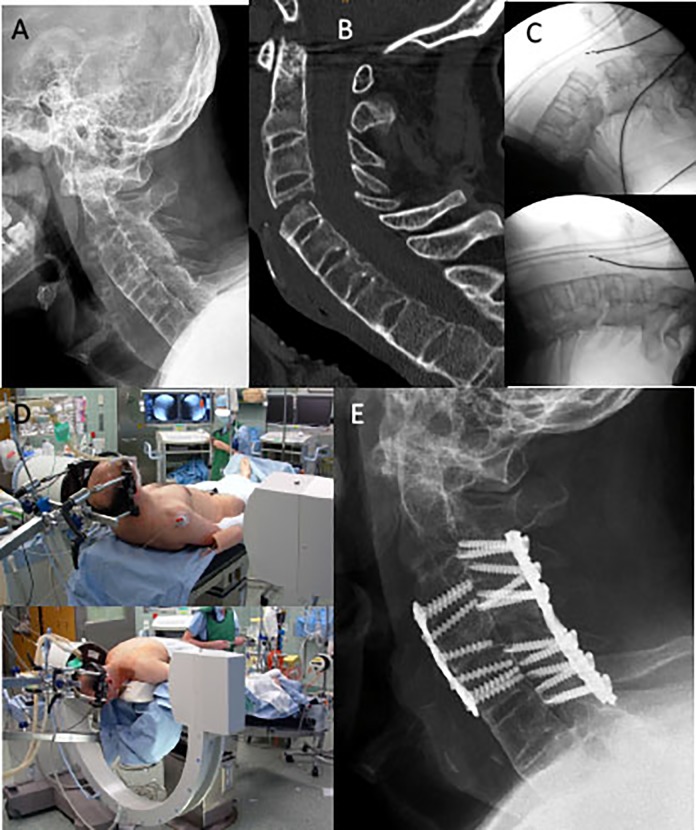
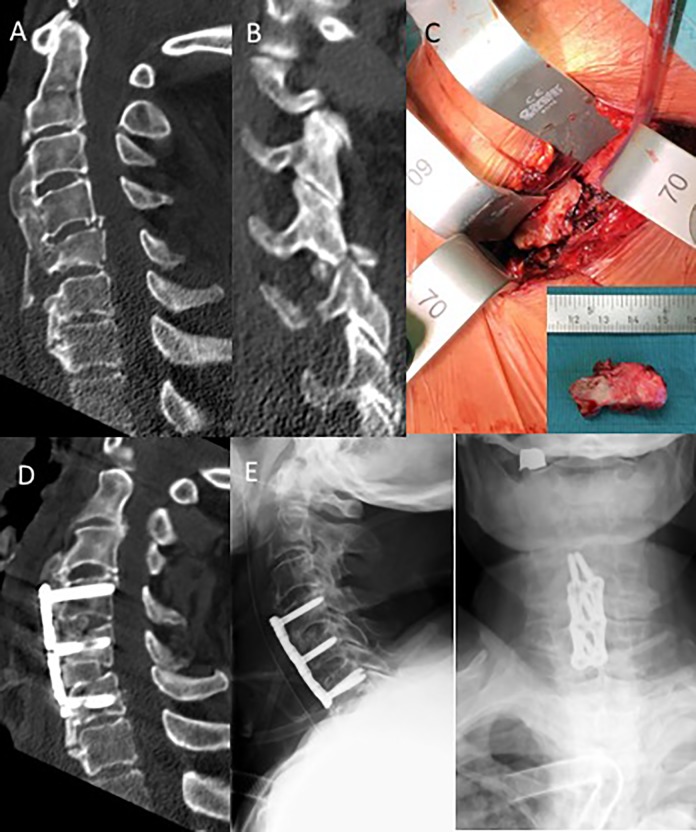
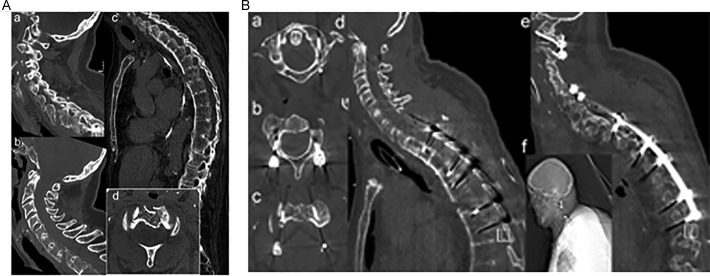
Results: Nondisplaced fractures can be missed easily using conventional X-rays. Thus, computed tomography (CT) scans are recommended for all trauma patients with ASD. In doubt or presence of any neurologic involvement additional magnetic resonance imaging (MRI) scans should be obtained. Spine precautions should be maintained all times and until definitive treatment (<24 h). Nonoperative fracture treatment is not recommended given the mechanical instability of the most commonly seen fracture patterns (AOSpine B- and C-type, M2) in patients with ASD and inherent high risk of secondary neurologic deterioration. For patients with ankylosing spondylitis (AS) or diffuse idiopathic hyperostosis (DISH) sustaining cervical spine fractures, a combined anterior-posterior instrumentation for fracture fixation is recommended. Closed reduction and patient positioning can be challenging in presence of preexisting kyphotic deformities. In the thoracolumbar (TL) spine, a posterior instrumentation extending 2 to 3 levels above and below the fracture level is recommended to maintain adequate reduction and stability until fracture healing. Minimally invasive percutaneous pedicle screws and cement augmentation can help to minimize the surgical trauma and strengthen the construct stability in patients with diminished minor bone quality (osteopenia, osteoporosis).
Conclusions: Current concepts, treatment options, and recommendations of the German Orthopedic Trauma Society-Spine Section for spinal fractures in the ankylosed spine have been outlined.
Keywords: DISH; Morbus Bechterew; Morbus Forestier; ankylosing spondylitis; cervical spine; complication; diffuse idiopathic skeletal hyperostosis; iatrogenic spine fracture; medical treatment; nonoperative fracture treatment; operative treatment; senile ankylosing hyperostosis; spinal fractures; thoracolumbar spine; trauma.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Is routine MRI of the spine necessary in trauma patients with ankylosing spinal disorders or is a CT scan sufficient?Spine J. 2019 Aug;19(8):1331-1339. doi: 10.1016/j.spinee.2019.03.004. Epub 2019 Mar 16. Spine J. 2019. PMID: 30890497
-
[Ankylosed spine fractures with spondylitis or diffuse idiopathic skeletal hyperostosis: diagnosis and complications].Rev Chir Orthop Reparatrice Appar Mot. 2004 Sep;90(5):456-65. doi: 10.1016/s0035-1040(04)70173-7. Rev Chir Orthop Reparatrice Appar Mot. 2004. PMID: 15502769 Review. French.
-
[Subaxial Cervical Spine Injuries: Treatment Recommendations of the German Orthopedic and Trauma Society].Z Orthop Unfall. 2017 Oct;155(5):556-566. doi: 10.1055/s-0043-110855. Epub 2017 Jul 20. Z Orthop Unfall. 2017. PMID: 28728206 German.
-
Spinal trauma in DISH and AS: is MRI essential following the detection of vertebral fractures on CT?Spine J. 2021 Apr;21(4):618-626. doi: 10.1016/j.spinee.2020.10.027. Epub 2020 Oct 30. Spine J. 2021. PMID: 33130303
-
Spine Fractures of Patients with Ankylosing Spondylitis and Diffuse Idiopathic Skeletal Hyperostosis: Fracture Severity and Injury-Related Mortality at a Level I Trauma Center.Asian Spine J. 2023 Jun;17(3):549-558. doi: 10.31616/asj.2022.0155. Epub 2023 Feb 13. Asian Spine J. 2023. PMID: 36775833 Free PMC article.
Cited by
-
Current status of short segment fixation in thoracolumbar spine injuries.J Clin Orthop Trauma. 2020 Sep-Oct;11(5):770-777. doi: 10.1016/j.jcot.2020.06.008. Epub 2020 Jun 26. J Clin Orthop Trauma. 2020. PMID: 32879564 Free PMC article. Review.
-
Conservative treatment for stable low-energy thoracolumbar vertebral fractures in nonfused segments among elderly patients with diffuse idiopathic skeletal hyperostosis: A matched case-control study.Medicine (Baltimore). 2019 Jun;98(24):e16032. doi: 10.1097/MD.0000000000016032. Medicine (Baltimore). 2019. PMID: 31192958 Free PMC article.
-
Korean treatment recommendations for patients with axial spondyloarthritis.J Rheum Dis. 2023 Jul 1;30(3):151-169. doi: 10.4078/jrd.2023.0025. J Rheum Dis. 2023. PMID: 37476674 Free PMC article. Review.
-
Surgical Stabilization of a Cervical Fracture in a Patient with Ankylosing Spondylitis in the Sitting Position.Cureus. 2020 Jan 10;12(1):e6625. doi: 10.7759/cureus.6625. Cureus. 2020. PMID: 31966941 Free PMC article.
-
Open versus minimally invasive fixation of thoracic and lumbar spine fractures in patients with ankylosing spinal diseases.Eur J Trauma Emerg Surg. 2022 Jun;48(3):2297-2307. doi: 10.1007/s00068-021-01756-3. Epub 2021 Aug 6. Eur J Trauma Emerg Surg. 2022. PMID: 34357408 Free PMC article.
References
-
- Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010;35:E458–E464. doi:10.1097/BRS.0b013e3181cc764f. - PubMed
-
- Forestier J, Lagier R. Ankylosing hyperostosis of the spine. Clin Orthop Relat Res. 1971;74:65–83. - PubMed
-
- Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology. 1976;119:559–568. doi:10.1148/119.3.559. - PubMed
-
- Cammisa M, De Serio A, Guglielmi G. Diffuse idiopathic skeletal hyperostosis. Eur J Radiol. 1998;27(suppl 1): S7–S11. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
