

Impact of Surgical Margin in Skull Base Surgery for Head and Neck Sarcomas
- PMID: 30210970
- PMCID: PMC6133685
- DOI: 10.1055/s-0037-1615816
Impact of Surgical Margin in Skull Base Surgery for Head and Neck Sarcomas
Abstract
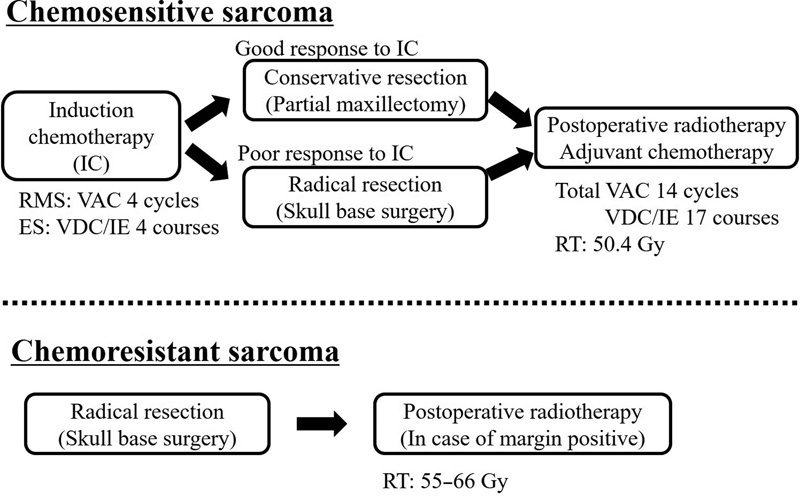
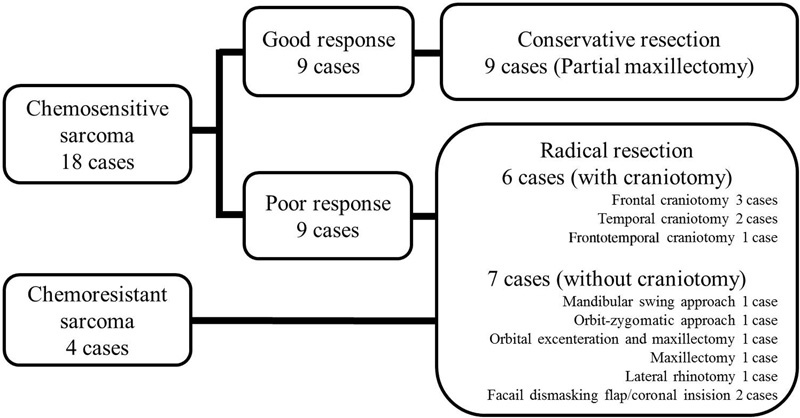
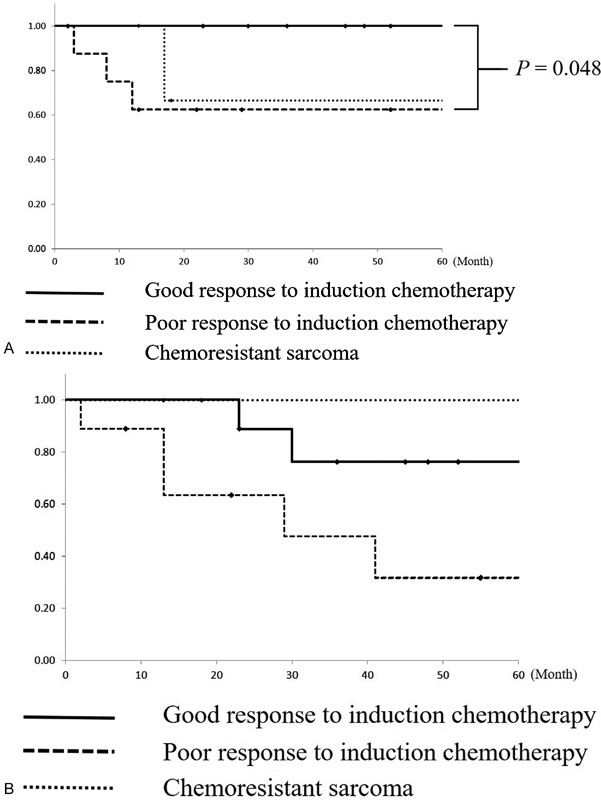
Objective This study aimed to determine the adequate resection margin in skull base surgery for head and neck sarcoma. Design We retrospectively reviewed 22 sarcomas with skull base invasion. Induction chemotherapy, followed by surgery and postoperative radiotherapy and adjuvant chemotherapy, was performed in 18 patients with chemosensitive sarcomas, and surgery with or without postoperative radiotherapy was performed in four patients with chemoresistant sarcomas. Radical resection was performed in patients with chemosensitive sarcomas with a poor response to induction chemotherapy and in patients with chemoresistant sarcomas. Conservative resection with close surgical margin was performed in patients with chemosensitive sarcomas with a good response to induction chemotherapy. Setting and Participants This single-centered retrospective study included patients from the National Cancer Center Hospital, Japan. Results The response to induction chemotherapy was significantly associated with the 3-year local control rate (LCR; good response versus poor response: 100% versus 63%, p = 0.048). Patients with a good response to chemotherapy had a favorable local prognosis even when the local therapy was conservative resection. In radical skull base surgery, patients whose surgical margins were classified as "wide margin positive" had significantly poorer 3-year LCR than did patients with "margin negative" or "micro margin positive" margins (25% versus 83%, p = 0.014). Conclusion Conservative resection with close surgical margins might be acceptable for chemosensitive sarcomas with a good response to chemotherapy. Resection margin status was an important predictive factor for local recurrence after radical skull base surgery. Microscopic microresidual tumor might be controlled by postoperative treatment.
Keywords: chemosensitivity; head and neck sarcoma; induction chemotherapy; skull base surgery; surgical margin.
Conflict of interest statement
Figures
References
-
- Montogomery P Q, Evans P HR, Gullane P J. London: Informa; 2009. Principles and Practice of Head and Neck Surgery and Oncology. 2nd ed.
-
- Fletcher C D. Distinctive soft tissue tumors of the head and neck. Mod Pathol. 2002;15(03):324–330. - PubMed
-
- O'Sullivan B, Bell R S, Bramwell V HC. Oxford: Oxford University Press; 2002. Sarcomas of the soft tissue; pp. 2495–2523.
-
- Arndt C A, Stoner J A, Hawkins D S et al.Vincristine, actinomycin, and cyclophosphamide compared with vincristine, actinomycin, and cyclophosphamide alternating with vincristine, topotecan, and cyclophosphamide for intermediate-risk rhabdomyosarcoma: children's oncology group study D9803. J Clin Oncol. 2009;27(31):5182–5188. - PMC - PubMed
-
- Grier H E, Krailo M D, Tarbell N J et al.Addition of ifosfamide and etoposide to standard chemotherapy for Ewing's sarcoma and primitive neuroectodermal tumor of bone. N Engl J Med. 2003;348(08):694–701. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
