

Creatine kinase, energy reserve, and hypertension: from bench to bedside
- PMID: 30211180
- PMCID: PMC6123196
- DOI: 10.21037/atm.2018.07.15
Creatine kinase, energy reserve, and hypertension: from bench to bedside
Abstract
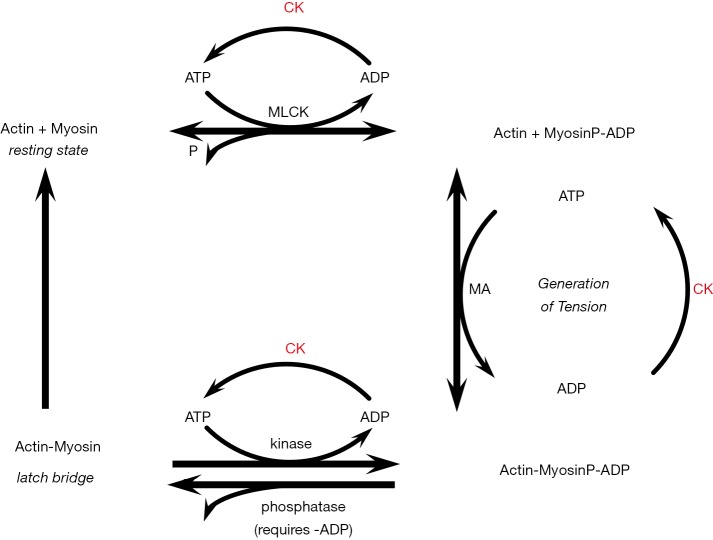
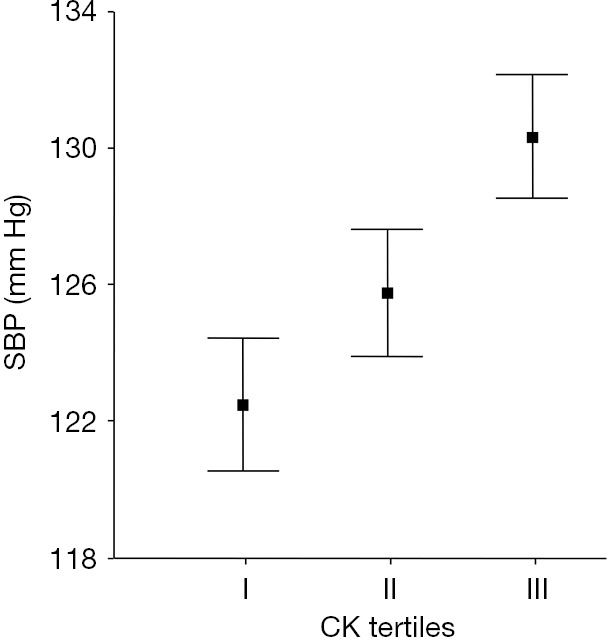
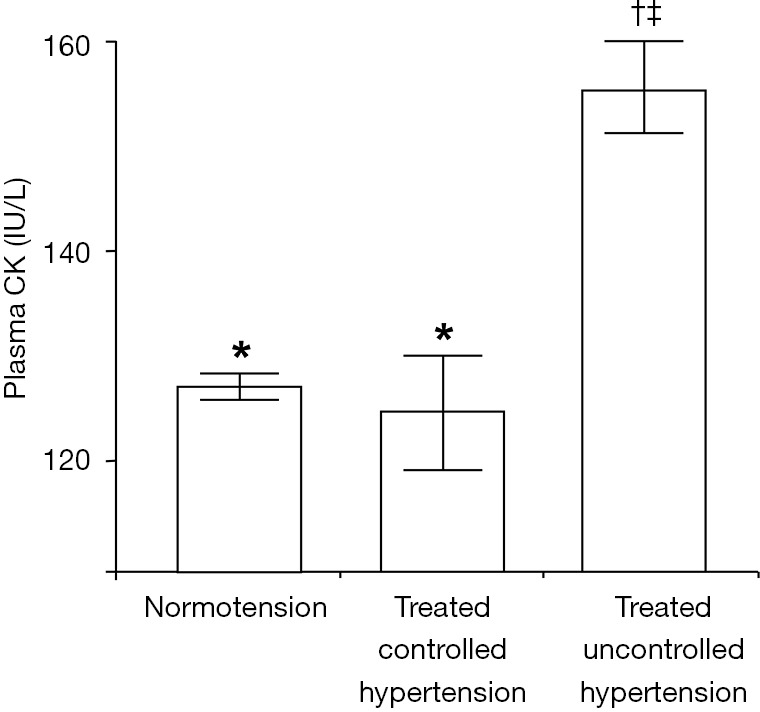
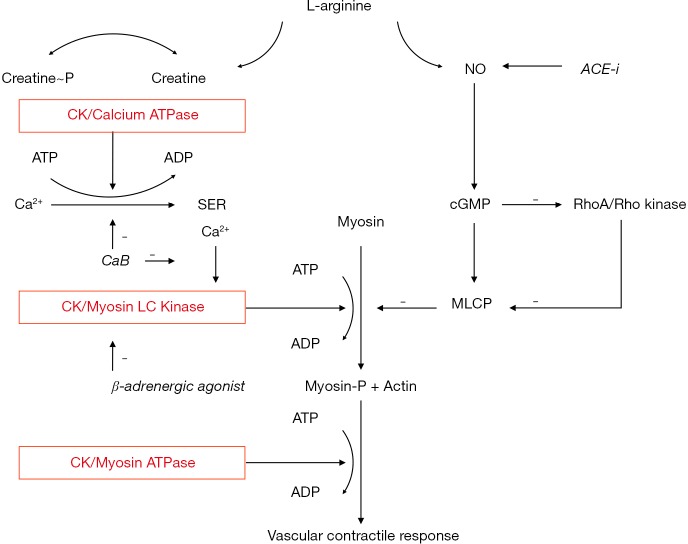
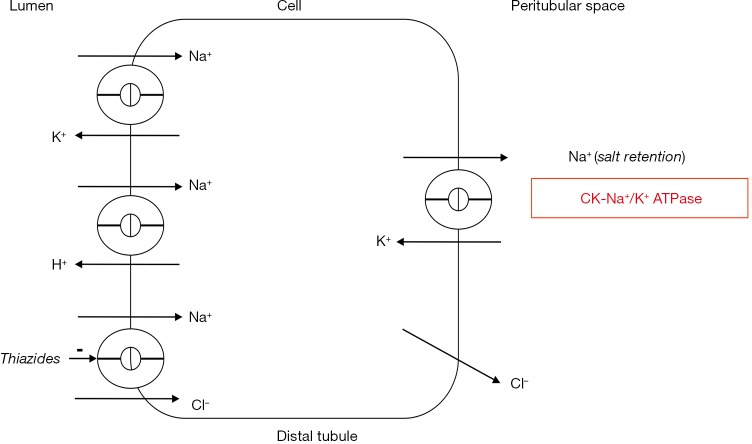
We hypothesized that human variation in the activity of the ATP regenerating enzyme creatine kinase (CK) activity affects hypertension and cardiovascular disease risk. CK is tightly bound close to ATP-utilizing enzymes including Ca2+-ATPase, myosin ATPase, and Na+/K+-ATPase, where it rapidly regenerates ATP from ADP, H+, and phosphocreatine. Thus, relatively high CK was thought to enhance ATP-demanding processes including resistance artery contractility and sodium retention, and reduce ADP-dependent functions. In a series of studies of our group and others, CK was linked to hypertension and bleeding risk. Plasma CK after rest, used as a surrogate measure for tissue CK, was associated with high blood pressure and failure of antihypertensive therapy in case-control and population studies. Importantly, high tissue CK preceded hypertension in animal models and in humans, and human vascular tissue CK gene expression was strongly associated with clinical blood pressure. In line with this, CK inhibition substantially reduced the contractility of human resistance arteries ex vivo. We also presented evidence that plasma CK reduced ADP-dependent platelet aggregation. In subsequent intervention studies, the oral competitive CK inhibitor beta-guanidinopropionic acid (GPA) reduced blood pressure in spontaneously hypertensive rats (SHRs), and a 1-week trial of sub-therapeutic dose GPA in healthy men was uneventful. Thus, based on theoretical concepts, evidence was gathered in laboratory, case-control, and population studies that high CK is associated with hypertension and with bleeding risk, potentially leading to a new mode of cardiovascular risk reduction with CK inhibition.
Keywords: ADP; Creatine kinase (CK); ancestry groups; bleeding; hypertension.
Conflict of interest statement
Conflicts of Interest: Lizzy M. Brewster is an inventor on NL patent WO/2012/138226 (filed).
Figures
Similar articles
-
The acute effect of beta-guanidinopropionic acid versus creatine or placebo in healthy men (ABC Trial): study protocol for a randomized controlled trial.Trials. 2015 Feb 22;16:56. doi: 10.1186/s13063-015-0581-9. Trials. 2015. PMID: 25888414 Free PMC article. Clinical Trial.
-
The acute effect of beta-guanidinopropionic acid versus creatine or placebo in healthy men (ABC-Trial): A randomized controlled first-in-human trial.Br J Clin Pharmacol. 2017 Dec;83(12):2626-2635. doi: 10.1111/bcp.13390. Epub 2017 Sep 20. Br J Clin Pharmacol. 2017. PMID: 28795416 Free PMC article. Clinical Trial.
-
Paradoxical Increase in Body Mass Induced by Beta-Guanidinopropionic Acid in Juvenile Spontaneously Hypertensive Rats.Cureus. 2021 Nov 9;13(11):e19394. doi: 10.7759/cureus.19394. eCollection 2021 Nov. Cureus. 2021. PMID: 34925996 Free PMC article.
-
The creatine kinase system and pleiotropic effects of creatine.Amino Acids. 2011 May;40(5):1271-96. doi: 10.1007/s00726-011-0877-3. Epub 2011 Mar 30. Amino Acids. 2011. PMID: 21448658 Free PMC article. Review.
-
The creatine kinase reaction: a simple reaction with functional complexity.Amino Acids. 2011 May;40(5):1363-7. doi: 10.1007/s00726-011-0856-8. Epub 2011 Mar 11. Amino Acids. 2011. PMID: 21394603 Review.
Cited by
-
Creatine kinase during non-ST-segment elevation acute coronary syndromes is associated with major bleeding.Open Heart. 2020 Dec;7(2):e001281. doi: 10.1136/openhrt-2020-001281. Open Heart. 2020. PMID: 33262195 Free PMC article. Clinical Trial.
-
Time-restricted eating with or without a low-carbohydrate diet improved myocardial status and thyroid function in individuals with metabolic syndrome: secondary analysis of a randomized clinical trial.BMC Med. 2024 Sep 4;22(1):362. doi: 10.1186/s12916-024-03595-6. BMC Med. 2024. PMID: 39227921 Free PMC article. Clinical Trial.
-
Creatine Kinase and Blood Pressure: A Systematic Review.Med Sci (Basel). 2019 Apr 9;7(4):58. doi: 10.3390/medsci7040058. Med Sci (Basel). 2019. PMID: 30970679 Free PMC article. Review.
-
Role of salvianolic acid B in the treatment of acute ischemic stroke: a systematic review and meta-analysis of animal models.Front Pharmacol. 2024 Dec 24;15:1479765. doi: 10.3389/fphar.2024.1479765. eCollection 2024. Front Pharmacol. 2024. PMID: 39776581 Free PMC article. Review.
-
Abnormal myocardial enzymes in the prediction of mortality and hypertension in COVID-19 patients: a retrospective study.Aging (Albany NY). 2022 Nov 2;14(21):8585-8594. doi: 10.18632/aging.204362. Epub 2022 Nov 2. Aging (Albany NY). 2022. PMID: 36326681 Free PMC article.
References
-
- Guyton AC. Arterial Pressure and Hypertension. Philadelphia, PA: W.B. Saunders, 1980.
-
- Folkow B, Hansson L Sivertson R. Structural vascular factors in the pathogeneisis of hypertension. In: Birkenhager WH, Reid JL, eds. Handbook of hypertension. Volume 1 Clinical aspects of essential hypertension. Amsterdam: Elsevier, 1983.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous