

The Diagnostic Value of Diffusion-Weighted Imaging in Differentiating Metastatic Lymph Nodes of Head and Neck Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 30213809
- PMCID: PMC7410724
- DOI: 10.3174/ajnr.A5813
The Diagnostic Value of Diffusion-Weighted Imaging in Differentiating Metastatic Lymph Nodes of Head and Neck Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
Abstract
Background: Accurate lymph node staging is crucial for proper treatment planning for metastasis in patients with head and neck squamous cell carcinoma.
Purpose: Our aim was to evaluate the diagnostic performance of DWI for differentiating metastatic cervical lymph nodes from benign cervical lymph nodes in patients with head and neck squamous cell carcinoma and to identify optimal cutoff values for ADC.
Data sources: A computerized literature search was performed to identify relevant original articles in Ovid MEDLINE and EMBASE.
Study selection: Studies evaluating the diagnostic performance of DWI for differentiating metastatic cervical lymph nodes from benign cervical lymph nodes were selected.
Data analysis: Diagnostic meta-analysis was conducted with a bivariate random-effects model, and a hierarchical summary receiver operating characteristic curve was obtained. Meta-regression was also performed.
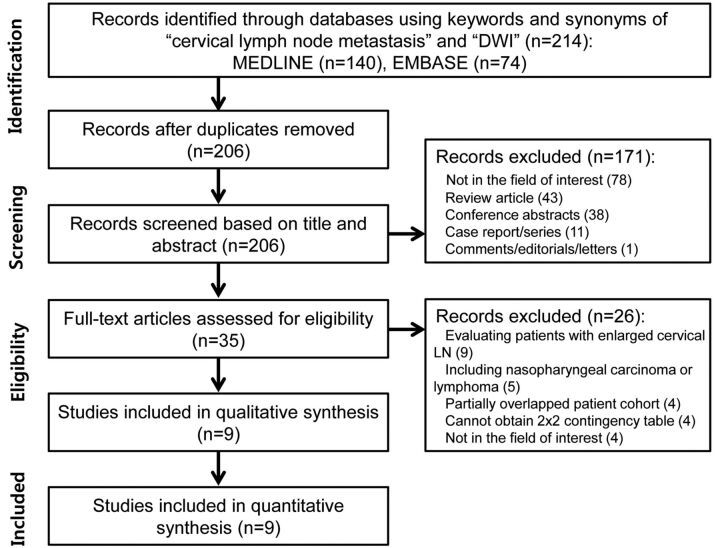
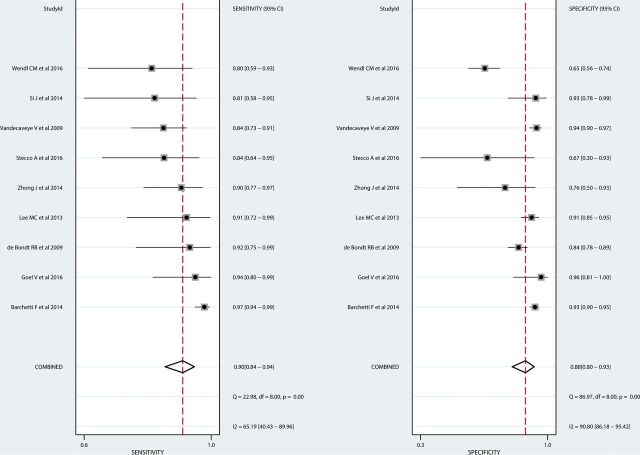
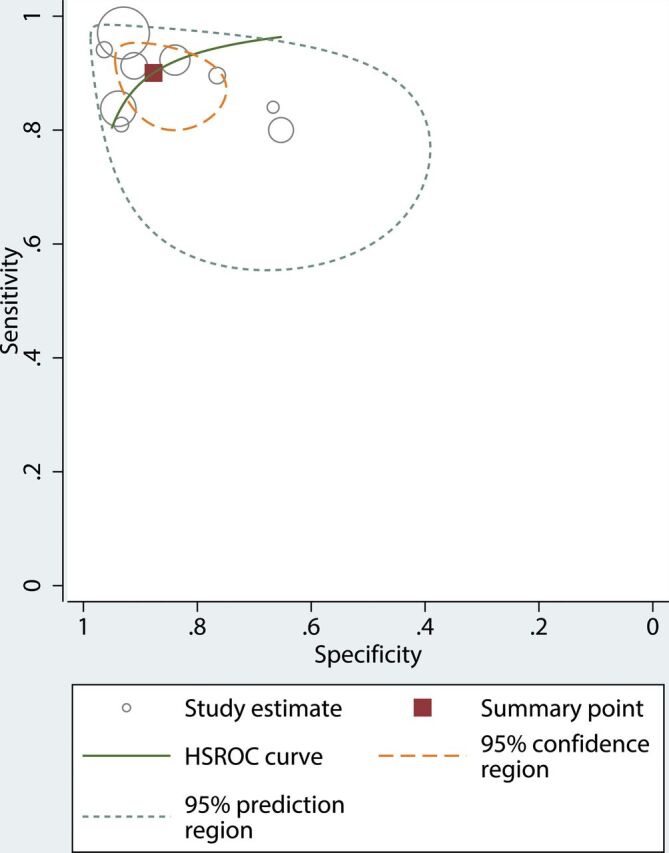
Data synthesis: Nine studies with 337 patients were included. In all studies, ADC values derived from metastatic lymph nodes were significantly lower than ADC values derived from benign lymph nodes. The median ADC cutoff value was 0.965 × 10-3 mm2/s. The pooled sensitivity and specificity for the diagnostic performance of DWI in differentiating metastatic lymph nodes from benign lymph nodes were 90% (95% CI, 84%-94%) and 88% (95% CI, 80%-93%), respectively. In the meta-regression, sensitivity was significantly higher in the studies using a 3-mm slice thickness (93% [95% CI, 88%-98%]) than in studies using a slice thickness of >3 mm (86% [95% CI, 77%-95%], P < .01).
Limitations: A small number of studies were included in our meta-analysis.
Conclusions: DWI demonstrated high diagnostic performance for differentiating metastatic lymph nodes from benign lymph nodes in patients with head and neck squamous cell carcinoma, and the median ADC cutoff value was 0.965 × 10-3 mm2/s. A 3-mm DWI slice thickness can provide a slight improvement in sensitivity.
© 2018 by American Journal of Neuroradiology.
Figures
Similar articles
-
Diffusion-Weighted Imaging (DWI) derived from PET/MRI for lymph node assessment in patients with Head and Neck Squamous Cell Carcinoma (HNSCC).Cancer Imaging. 2020 Aug 8;20(1):56. doi: 10.1186/s40644-020-00334-x. Cancer Imaging. 2020. PMID: 32771060 Free PMC article.
-
Differentiation of lymphomatous, metastatic, and non-malignant lymphadenopathy in the neck with quantitative diffusion-weighted imaging: systematic review and meta-analysis.Neuroradiology. 2019 Aug;61(8):897-910. doi: 10.1007/s00234-019-02236-7. Epub 2019 Jun 7. Neuroradiology. 2019. PMID: 31175398
-
Evaluating the Elasticity of Metastatic Cervical Lymph Nodes in Head and Neck Squamous Cell Carcinoma Patients Using DWI-based Virtual MR Elastography.Magn Reson Med Sci. 2024 Jan 1;23(1):49-55. doi: 10.2463/mrms.mp.2022-0082. Epub 2022 Dec 16. Magn Reson Med Sci. 2024. PMID: 36529497 Free PMC article.
-
Evaluation of the diagnostic performance of apparent diffusion coefficient (ADC) values on diffusion-weighted magnetic resonance imaging (DWI) in differentiating between benign and metastatic lymph nodes in cases of cholangiocarcinoma.Abdom Radiol (NY). 2019 Feb;44(2):473-481. doi: 10.1007/s00261-018-1742-6. Abdom Radiol (NY). 2019. PMID: 30151713
-
Diffusion Weighted Imaging for the Assessment of Lymph Node Metastases in Women with Cervical Cancer: A Meta-analysis of the Apparent Diffusion Coefficient Values.Acad Radiol. 2025 Mar;32(3):1465-1475. doi: 10.1016/j.acra.2024.09.020. Epub 2024 Sep 25. Acad Radiol. 2025. PMID: 39327136 Review.
Cited by
-
ADC Values of Cytologically Benign and Cytologically Malignant 18 F-FDG PET-Positive Lymph Nodes of Head and Neck Squamous Cell Carcinoma.Cancers (Basel). 2022 Aug 20;14(16):4019. doi: 10.3390/cancers14164019. Cancers (Basel). 2022. PMID: 36011013 Free PMC article.
-
Diffusion-Weighted Imaging (DWI) derived from PET/MRI for lymph node assessment in patients with Head and Neck Squamous Cell Carcinoma (HNSCC).Cancer Imaging. 2020 Aug 8;20(1):56. doi: 10.1186/s40644-020-00334-x. Cancer Imaging. 2020. PMID: 32771060 Free PMC article.
-
Characterization of pediatric head and neck masses with quantitative analysis of diffusion-weighted imaging and measurement of apparent diffusion coefficients.Indian J Radiol Imaging. 2020 Oct-Dec;30(4):473-481. doi: 10.4103/ijri.IJRI_129_19. Epub 2021 Jan 13. Indian J Radiol Imaging. 2020. PMID: 33737777 Free PMC article.
-
Lack of restricted diffusion in MR imaging as a potential differentiating tool of reactive lymph node in cat scratch disease from lymphoma or abscess.Radiol Case Rep. 2020 Jun 9;15(8):1180-1183. doi: 10.1016/j.radcr.2020.05.017. eCollection 2020 Aug. Radiol Case Rep. 2020. PMID: 32547675 Free PMC article.
-
Differentiation of lymphomatous, metastatic, and non-malignant lymphadenopathy in the neck with quantitative diffusion-weighted imaging: systematic review and meta-analysis.Neuroradiology. 2019 Aug;61(8):897-910. doi: 10.1007/s00234-019-02236-7. Epub 2019 Jun 7. Neuroradiology. 2019. PMID: 31175398
References
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Head and Neck Cancers V.2.2017. https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf. Accessed January 23, 2018 To view the most recent and complete version of the guidelines, National Comprehensive Cancer Network®, NCCN®, NCCN Guidelines®, and all other NCCN content that are trademarks owned by the National Comprehensive Cancer Network, Inc, see www.nccn.org. Accessed January 23, 2018
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources