

Clinical Evaluation of Highly Accelerated Compressed Sensing Time-of-Flight MR Angiography for Intracranial Arterial Stenosis
- PMID: 30213812
- PMCID: PMC7410741
- DOI: 10.3174/ajnr.A5786
Clinical Evaluation of Highly Accelerated Compressed Sensing Time-of-Flight MR Angiography for Intracranial Arterial Stenosis
Abstract
Background and purpose: Time-of-flight MR angiography is the preferred imaging technique to assess intracranial arterial stenosis but is limited by a relatively long acquisition time. Compressed sensing provides an innovative approach in undersampling k-space to minimize the data-acquisition time. We aimed to evaluate the diagnostic accuracy of compressed sensing TOF for detecting intracranial arterial stenosis by comparison with conventional parallel imaging TOF-MRA.
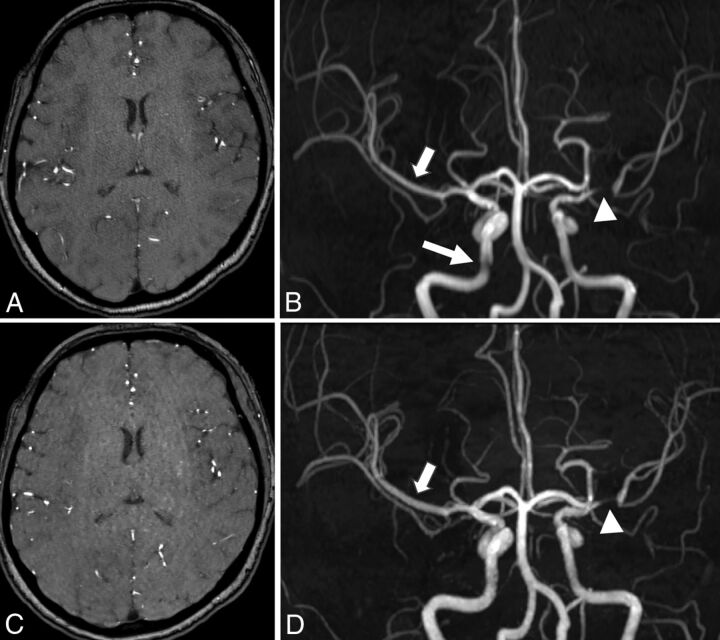
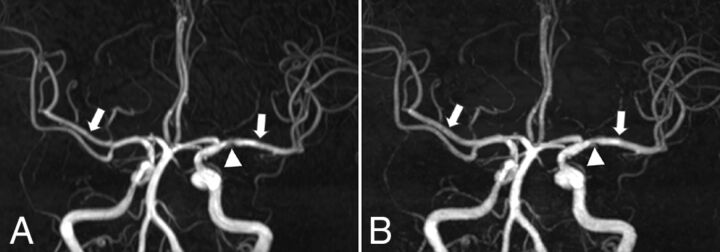
Materials and methods: Compressed sensing TOF and parallel imaging TOF were performed in 22 patients with intracranial arterial stenosis. The MRA scan times were 2 minutes and 31 seconds and 4 minutes and 48 seconds for compressed sensing TOF and parallel imaging TOF, respectively. The reconstructed resolutions were 0.4 × 0.4 × 0.4 and 0.4 × 0.4 × 0.6 mm3 for compressed sensing TOF and parallel imaging TOF, respectively. The diagnostic quality of the images and visibility of the stenoses were independently ranked by 2 neuroradiologists blinded to the type of method and were compared using the Wilcoxon signed rank test. Concordance was calculated with the Cohen κ. Edge sharpness of the arteries and the luminal stenosis ratio were analyzed and compared using a paired-sample t test.
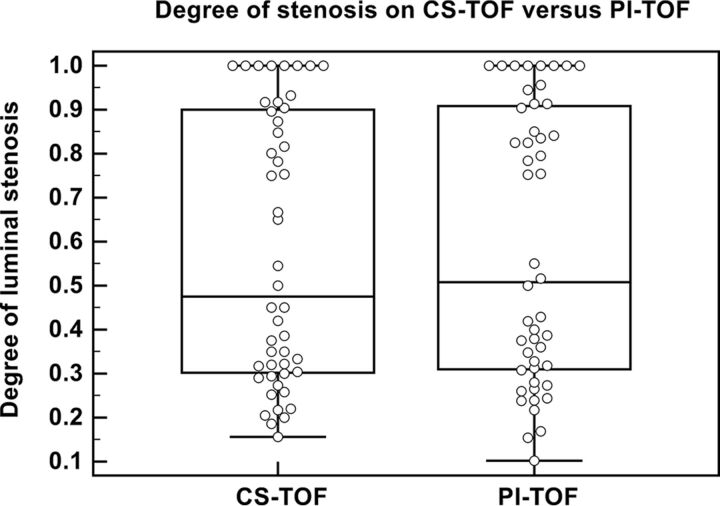
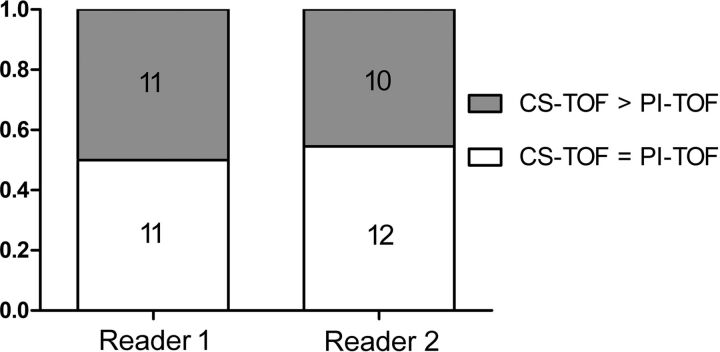
Results: The interrater agreement was good to excellent. Compressed sensing TOF resulted in image quality comparable with that of parallel imaging TOF but boosted confidence in diagnosing arterial stenoses (P = .025). The edge sharpness of the intracranial arteries for compressed sensing TOF was significantly higher than that for parallel imaging TOF (P < .001). The luminal stenosis ratio on compressed sensing TOF showed no significant difference compared with that on parallel imaging TOF.
Conclusions: Compressed sensing TOF both remarkably reduced the scan time and provided adequate image quality for the diagnosis of intracranial arterial stenosis.
© 2018 by American Journal of Neuroradiology.
Figures
References
-
- Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, et al. ; American Heart Association Statistics Committee, Stroke Statistics Subcommittee. Heart disease and stroke statistics: 2016 update—a report from the American Heart Association. Circulation 2016;133:e38–360 10.1161/CIR.0000000000000350 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources