

Genomic and phenotypic delineation of congenital microcephaly
- PMID: 30214071
- PMCID: PMC6986385
- DOI: 10.1038/s41436-018-0140-3
Genomic and phenotypic delineation of congenital microcephaly
Abstract
Purpose: Congenital microcephaly (CM) is an important birth defect with long term neurological sequelae. We aimed to perform detailed phenotypic and genomic analysis of patients with Mendelian forms of CM.
Methods: Clinical phenotyping, targeted or exome sequencing, and autozygome analysis.
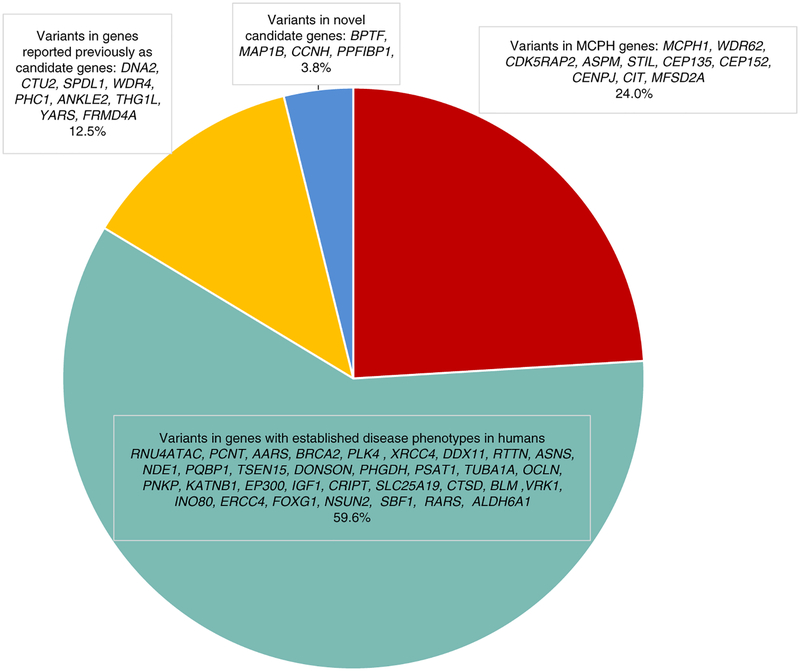
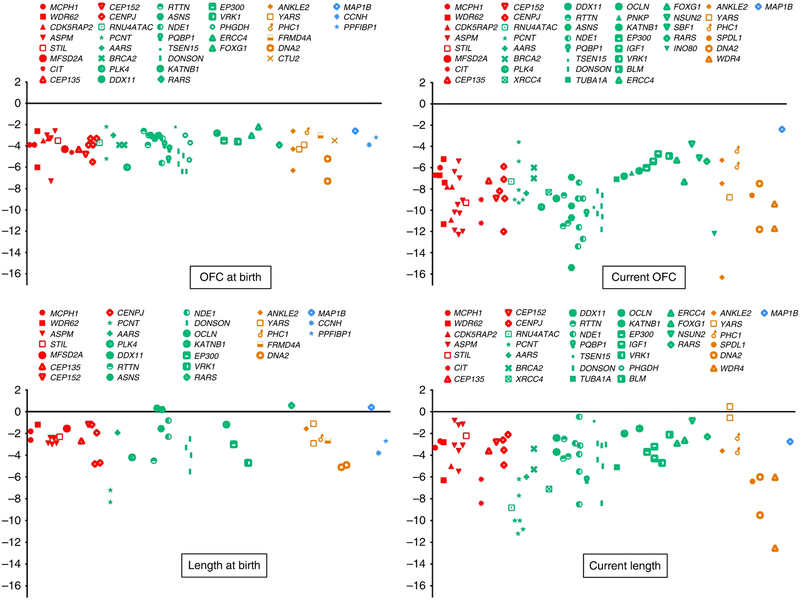
Results: We describe 150 patients (104 families) with 56 Mendelian forms of CM. Our data show little overlap with the genetic causes of postnatal microcephaly. We also show that a broad definition of primary microcephaly -as an autosomal recessive form of nonsyndromic CM with severe postnatal deceleration of occipitofrontal circumference-is highly sensitive but has a limited specificity. In addition, we expand the overlap between primary microcephaly and microcephalic primordial dwarfism both clinically (short stature in >52% of patients with primary microcephaly) and molecularly (e.g., we report the first instance of CEP135-related microcephalic primordial dwarfism). We expand the allelic and locus heterogeneity of CM by reporting 37 novel likely disease-causing variants in 27 disease genes, confirming the candidacy of ANKLE2, YARS, FRMD4A, and THG1L, and proposing the candidacy of BPTF, MAP1B, CCNH, and PPFIBP1.
Conclusion: Our study refines the phenotype of CM, expands its genetics heterogeneity, and informs the workup of children born with this developmental brain defect.
Keywords: CNTRL; autozygome; dwarfism; primary microcephaly.
Conflict of interest statement
DISCLOSURE
The authors declare no conflicts of interest.
Figures

References
-
- Ashwal S, Michelson D, Plawner L, Dobyns WB. Practice parameter: evaluation of the child with microcephaly (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2009;73:887–897. - PMC - PubMed
-
- Alcantara D and O’driscoll M, 2014, June. Congenital microcephaly. In American Journal of Medical Genetics Part C: Seminars in Medical Genetics 2014;166:124–139. - PubMed
-
- Krauss MJ, Morrissey AE, Winn HN, Amon E, Leet TL. Microcephaly: an epidemiologic analysis. Am J Obstet Gynecol 2003;188: 1484–1490. - PubMed
-
- Wollnik B A common mechanism for microcephaly. Nat Genet 2010;42:923–924. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
