

Scleral buckling in the management of rhegmatogenous retinal detachment: patient selection and perspectives
- PMID: 30214145
- PMCID: PMC6124476
- DOI: 10.2147/OPTH.S153717
Scleral buckling in the management of rhegmatogenous retinal detachment: patient selection and perspectives
Abstract
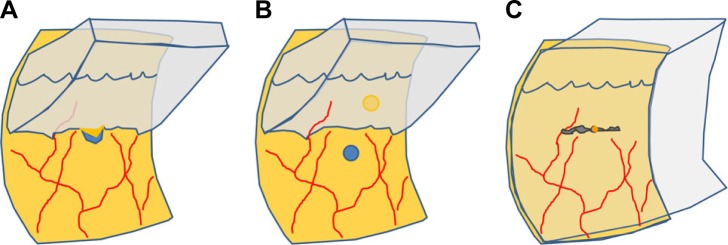
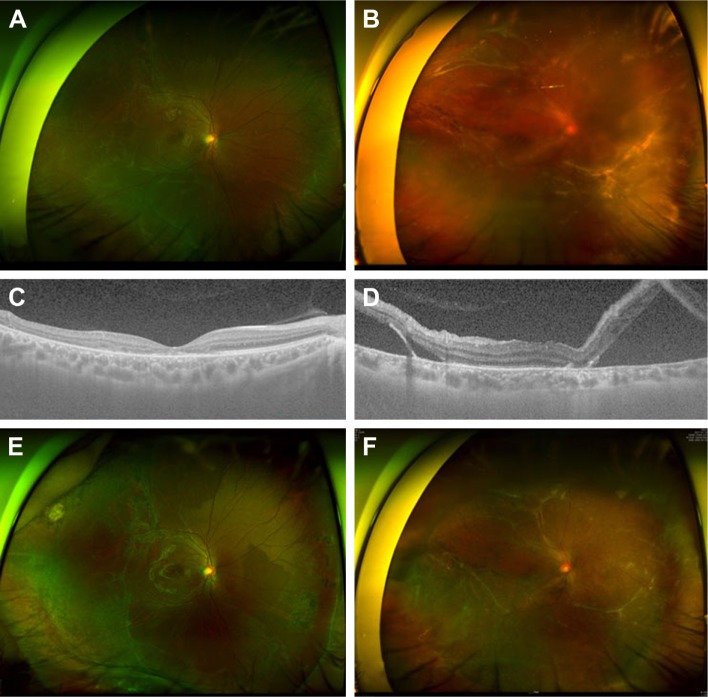
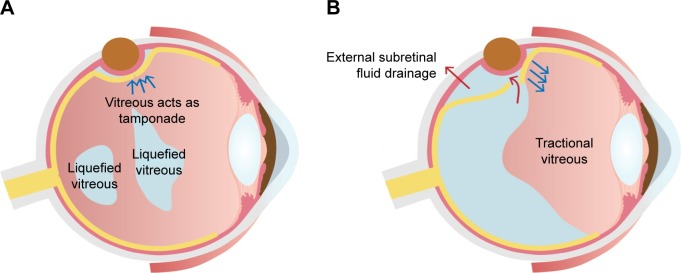
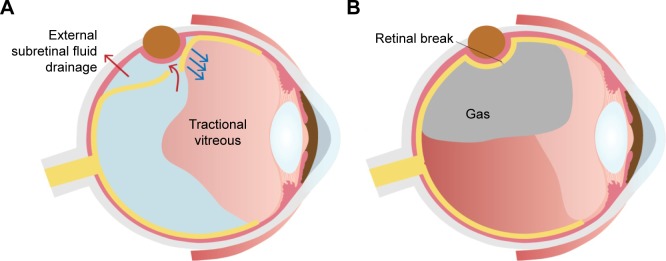
Although the technique of pars plana vitrectomy (PPV) develops rapidly, scleral buckling (SB) has several advantages over PPV for rhegmatogenous retinal detachment (RRD), including early visual rehabilitation and prevention of cataract progression. It is recommended to select the primary procedure for RRD by considering the advantages and disadvantages of each procedure based on the patient status. The vitreous body status affects the features of RRD. Vitreous liquefaction is an age-dependent process, resulting in the development of posterior vitreous detachment (PVD). RRD is usually associated with PVD, typically presenting with a retinal tear, strong vitreoretinal traction, and bullous detachment. In contrast, RRD may develop without PVD, and typically presents with a small atrophic hole, shallow detachment, and slow progression. RRD with less liquefied vitreous and no PVD can be managed successfully with SB alone even in the presence of subretinal strand as less liquefied vitreous acts as bio-tamponade blocking fluid passage. The strong traction induced by PVD and bullous detachment in an eye with extensively liquefied vitreous reduces the success rate of SB. PPV is gaining popularity as the primary procedure for RRD, especially in eyes with retinal tears, PVD, or pseudophakia. Nevertheless, SB remains the preferred procedure in young phakic patients without PVD.
Keywords: age; myopia; posterior vitreous detachment; rhegmatogenous retinal detachment; scleral buckling; vitreous.
Conflict of interest statement
Disclosure Lee JE is a consultant for Allergan, Bayer, and Novartis, and received honorarium from Alcon, Allergan, Bayer, and Novartis. The other authors report no conflicts of interest in this work.
Figures

Similar articles
-
Postoperative complications after successful primary rhegmatogenous retinal detachment repair.BMC Ophthalmol. 2023 Feb 24;23(1):77. doi: 10.1186/s12886-023-02824-5. BMC Ophthalmol. 2023. PMID: 36829144 Free PMC article.
-
The fellow eye of patients with phakic rhegmatogenous retinal detachment from atrophic holes of lattice degeneration without posterior vitreous detachment.Br J Ophthalmol. 2004 Nov;88(11):1400-2. doi: 10.1136/bjo.2004.043240. Br J Ophthalmol. 2004. PMID: 15489481 Free PMC article.
-
Preoperative B-scan ultrasonography of the vitreoretinal interface in phakic patients undergoing rhegmatogenous retinal detachment repair and its prognostic significance.Graefes Arch Clin Exp Ophthalmol. 2007 Sep;245(9):1295-301. doi: 10.1007/s00417-007-0541-5. Epub 2007 Feb 21. Graefes Arch Clin Exp Ophthalmol. 2007. PMID: 17318570
-
Scleral Buckling: A Look at the Past, Present and Future in View of Recent Findings on the Importance of Photoreceptor Re-Alignment Following Retinal Re-Attachment.Clin Ophthalmol. 2022 Jun 16;16:1971-1984. doi: 10.2147/OPTH.S359309. eCollection 2022. Clin Ophthalmol. 2022. PMID: 35733617 Free PMC article. Review.
-
Historical, Current and Future Approaches to Surgery for Rhegmatogenous Retinal Detachment.Tohoku J Exp Med. 2019 Jul;248(3):159-168. doi: 10.1620/tjem.248.159. Tohoku J Exp Med. 2019. PMID: 31308289 Review.
Cited by
-
Vitreous function and intervention of it with vitrectomy and other modalities.Int J Ophthalmol. 2022 Jun 18;15(6):857-867. doi: 10.18240/ijo.2022.06.02. eCollection 2022. Int J Ophthalmol. 2022. PMID: 35814889 Free PMC article.
-
Wide-angled endoillumination vs traditional scleral buckling surgery for retinal detachment - a comparative study.Clin Ophthalmol. 2019 Feb 8;13:287-293. doi: 10.2147/OPTH.S182751. eCollection 2019. Clin Ophthalmol. 2019. PMID: 30804661 Free PMC article.
-
Fortified Barrier Laser On The Vitreous Base In Vitrectomy For Rhegmatogenous Retinal Detachment.Clin Ophthalmol. 2019 Oct 31;13:2127-2133. doi: 10.2147/OPTH.S223415. eCollection 2019. Clin Ophthalmol. 2019. PMID: 31802842 Free PMC article.
-
The impact of the COVID-19 Pandemic on rhegmatogenous retinal detachment treatment patterns.BMC Ophthalmol. 2021 Oct 19;21(1):372. doi: 10.1186/s12886-021-02127-7. BMC Ophthalmol. 2021. PMID: 34666710 Free PMC article.
-
Scleral structure and biomechanics.Prog Retin Eye Res. 2020 Jan;74:100773. doi: 10.1016/j.preteyeres.2019.100773. Epub 2019 Aug 11. Prog Retin Eye Res. 2020. PMID: 31412277 Free PMC article. Review.
References
-
- Mitry D, Fleck BW, Wright AF, Campbell H, Charteris DG. Pathogenesis of rhegmatogenous retinal detachment: predisposing anatomy and cell biology. Retina. 2010;30(10):1561–1572. - PubMed
-
- Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678–684. - PubMed
-
- Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures. I. Surgical techniques and management. AMA Arch Ophthalmol. 1957;58(6):797–811. - PubMed
-
- Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813–820. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
