

A combination of SOFA score and biomarkers gives a better prediction of septic AKI and in-hospital mortality in critically ill surgical patients: a pilot study
- PMID: 30214469
- PMCID: PMC6131912
- DOI: 10.1186/s13017-018-0202-5
A combination of SOFA score and biomarkers gives a better prediction of septic AKI and in-hospital mortality in critically ill surgical patients: a pilot study
Abstract
Background: Sepsis is a syndrome characterized by a constellation of clinical manifestations and a significantly high mortality rate in the surgical intensive care unit (ICU). It is frequently complicated by acute kidney injury (AKI), which, in turn, increases the risk of mortality. Therefore, it is of paramount importance to identify those septic patients at risk for the development of AKI and mortality. The objective of this pilot study was to evaluate several different biomarkers, including NGAL, calprotectin, KIM-1, cystatin C, and GDF-15, along with SOFA scores, in predicting the development of septic AKI and associated in-hospital mortality in critically ill surgical patients.
Methods: Patients admitted to the surgical ICU were prospectively enrolled, having given signed informed consent. Their blood and urine samples were obtained and subjected to enzyme-linked immunosorbent assay (ELISA) to determine the levels of various novel biomarkers. The clinical data and survival outcome were recorded and analyzed.
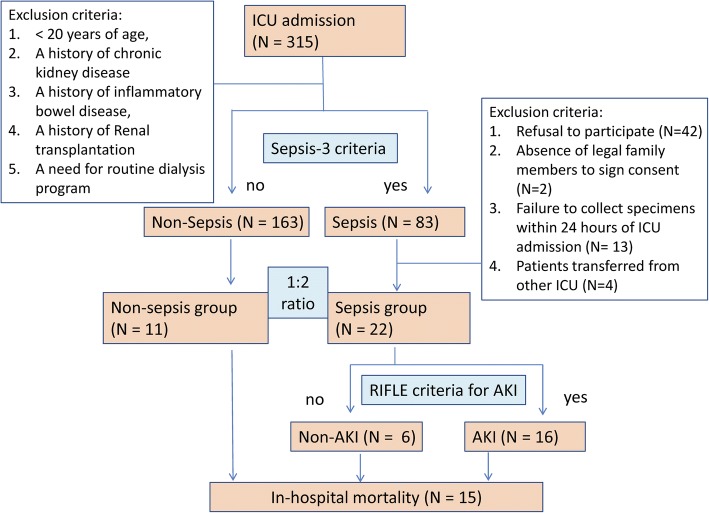
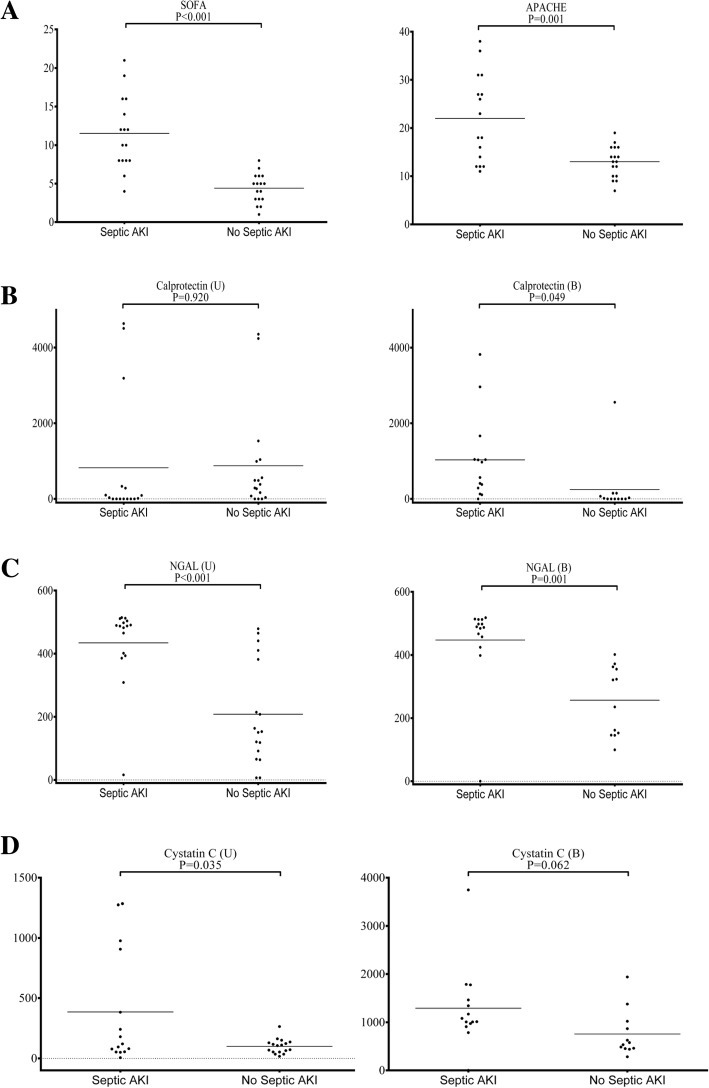
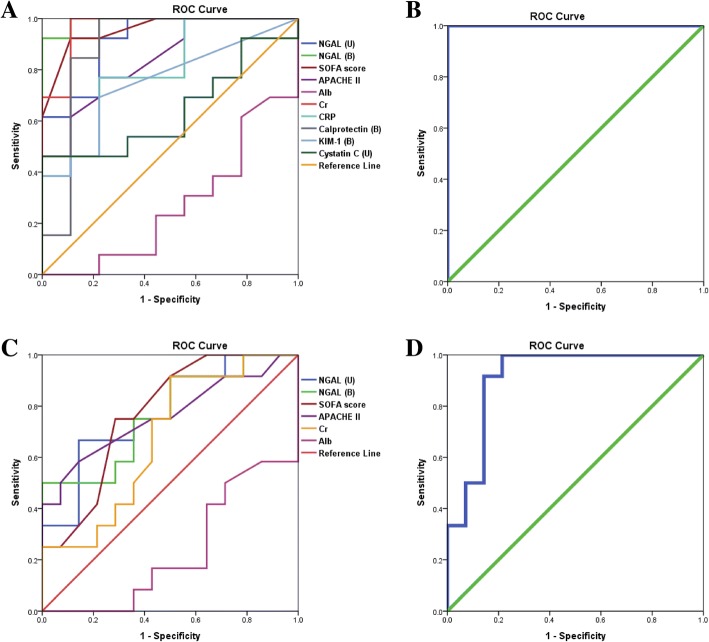
Results: A total of 33 patients were enrolled in the study. Most patients received surgery prior to ICU admission, with abdominal surgery being the most common type of procedure (27 patients (81.8%)). In the study, 22 patients had a diagnosis of sepsis with varying degrees of AKI, while the remaining 11 were free of sepsis. Statistical analysis demonstrated that in patients with septic AKI versus those without, the following were significantly higher: serum NGAL (447.5 ± 35.7 ng/mL vs. 256.5 ± 31.8 ng/mL, P value 0.001), calprotectin (1030.3 ± 298.6 pg/mL vs. 248.1 ± 210.7 pg/mL, P value 0.049), urinary NGAL (434.2 ± 31.5 ng/mL vs. 208.3 ± 39.5 ng/mL, P value < 0.001), and SOFA score (11.5 ± 1.2 vs. 4.4 ± 0.5, P value < 0.001). On the other hand, serum NGAL (428.2 ± 32.3 ng/mL vs. 300.4 ± 44.3 ng/mL, P value 0.029) and urinary NGAL (422.3 ± 33.7 ng/mL vs. 230.8 ± 42.2 ng/mL, P value 0.001), together with SOFA scores (10.6 ± 1.4 vs. 5.6 ± 0.8, P value 0.003), were statistically higher in cases of in-hospital mortality. A combination of serum NGAL, urinary NGAL, and SOFA scores could predict in-hospital mortality with an AUROC of 0.911.
Conclusions: This pilot study demonstrated a promising panel that allows an early diagnosis, high sensitivity, and specificity and a prognostic value for septic AKI and in-hospital mortality in surgical ICU. Further study is warranted to validate our findings.
Keywords: AKI; Acute kidney injury; Calprotectin; Critically ill patients; Intensive care unit; Mortality; NGAL; SOFA score; Sepsis; Surgical ICU.
Conflict of interest statement
This study was approved by the Institutional Review Boards (CGMH IRB No. 103-2722A3) of Chang Gung Memorial Hospital (CGMH). Written informed consent was obtained from all individuals who agreed to participate in the study.Consent to publish has been obtained from the participants (or legal parent or guardian for children) to report individual patient data.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
