

Flexible versus rigid endoscopy in the management of esophageal foreign body impaction: systematic review and meta-analysis
- PMID: 30214470
- PMCID: PMC6134522
- DOI: 10.1186/s13017-018-0203-4
Flexible versus rigid endoscopy in the management of esophageal foreign body impaction: systematic review and meta-analysis
Abstract
Background: Foreign body (FB) impaction accounts for 4% of emergency endoscopies in clinical practice. Flexible endoscopy (FE) is recommended as the first-line therapeutic option because it can be performed under sedation, is cost-effective, and is well tolerated. Rigid endoscopy (RE) under general anesthesia is less used but may be advantageous in some circumstances. The aim of the study was to compare the efficacy and safety of FE and RE in esophageal FB removal.
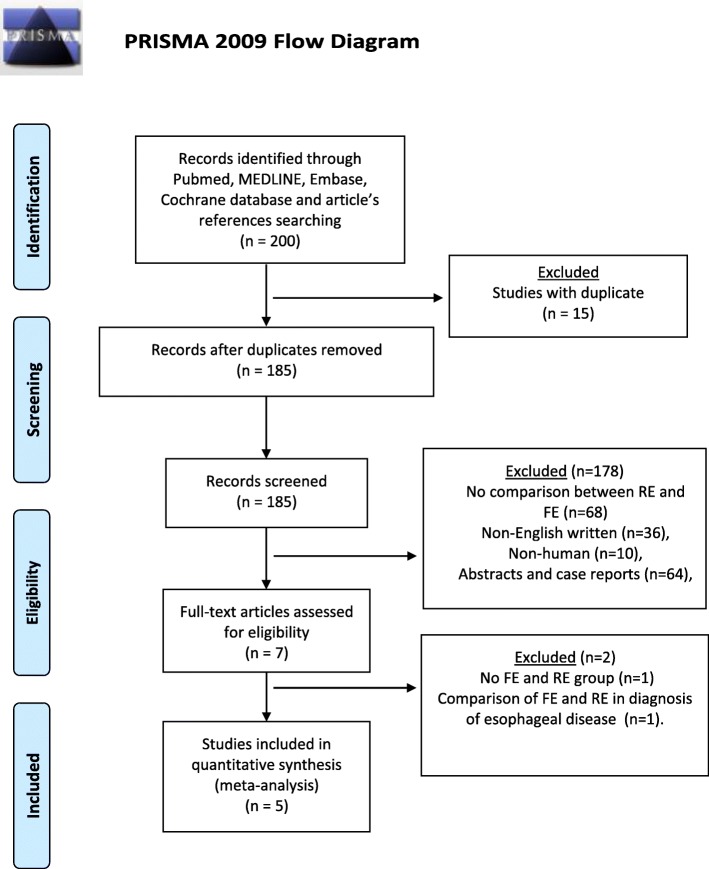
Methods: PubMed, MEDLINE, Embase, and Cochrane databases were consulted matching the terms "Rigid endoscopy AND Flexible endoscopy AND foreign bod*". Pooled effect measures were calculated using an inverse-variance weighted or Mantel-Haenszel in random effects meta-analysis. Heterogeneity was evaluated using I2 index and Cochrane Q test.
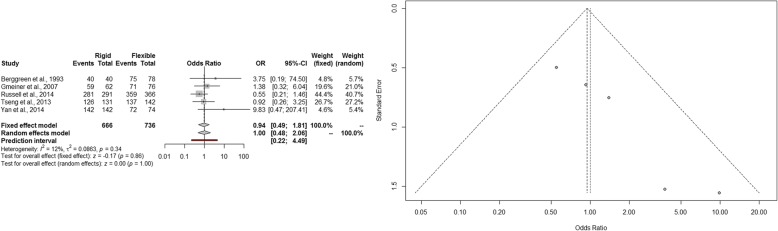
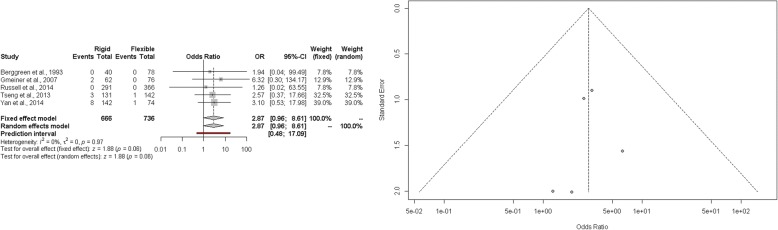
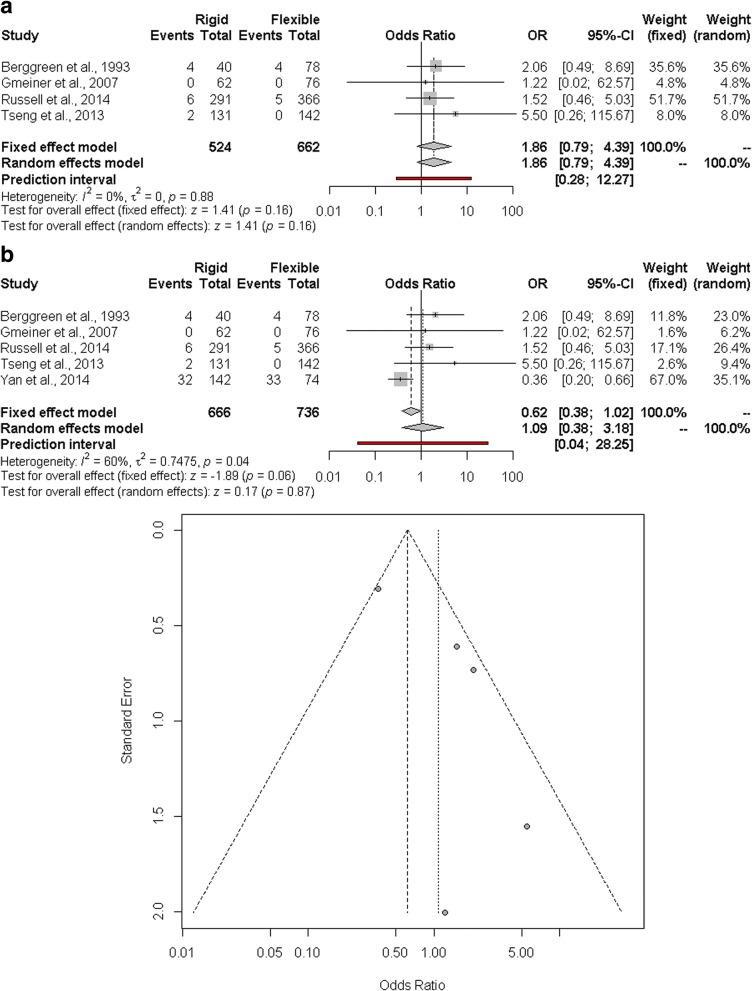
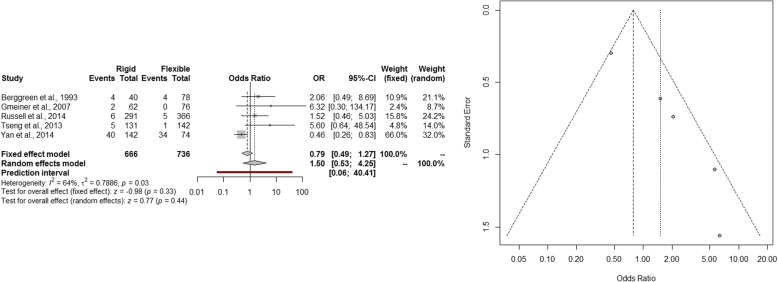
Results: Five observational cohort studies, published between 1993 and 2015, matched the inclusion criteria. One thousand four hundred and two patients were included; FE was performed in 736 patients and RE in 666. Overall, 101 (7.2%) complications occurred. The most frequent complications were mucosal erosion (26.7%), mucosal edema (18.8%), and iatrogenic esophageal perforations (10.9%). Compared to FE, the estimated RE pooled success OR was 1.00 (95% CI 0.48-2.06; p = 1.00). The pooled OR of iatrogenic perforation, other complications, and overall complications were 2.87 (95% CI 0.96-8.61; p = 0.06), 1.09 (95% CI 0.38-3.18; p = 0.87), and 1.50 (95% CI 0.53-4.25; p = 0.44), respectively. There was no mortality.
Conclusions: FE and RE are equally safe and effective for the removal of esophageal FB. To provide a tailored or crossover approach, patients should be managed in multidisciplinary centers where expertise in RE is also available. Formal training and certification in RE should probably be re-evaluated.
Keywords: Esophageal foreign body; Flexible endoscopy; Foreign body impaction; Iatrogenic esophageal perforation; Rigid endoscopy.
Conflict of interest statement
No ethical approval or consent to participate was required for this review.Not applicableThe authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Sugawa C. Endoscopic management of foreign bodies in the upper gastrointestinal tract: a review. World J Gastrointest Endosc. 2014;6:–475 Available from: http://www.wjgnet.com/1948-5190/full/v6/i10/475.htm. Accessed 29 June 2018. - PMC - PubMed
-
- Wyllie R. Foreign bodies in the gastrointestinal tract. Curr Opin Pediatr. 2006;18:563–4 Oct [cited 2018 Jun 25]; Available frome: https://insights.ovid.com/crossref?an=00008480-200610000-00015. Accessed 29 June 2018. - PubMed
-
- Webb WA. Management of foreign bodies of the upper gastrointestinal tract. Gastroenterology. 1988 ;94:204–16. [cited 2018 Jun 21] Available from: http://linkinghub.elsevier.com/retrieve/pii/0016508588906324 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
