

Diagnostic utility of eight-channel EEG for detecting generalized or hemispheric seizures and rhythmic periodic patterns
- PMID: 30215011
- PMCID: PMC6133909
- DOI: 10.1016/j.cnp.2018.03.001
Diagnostic utility of eight-channel EEG for detecting generalized or hemispheric seizures and rhythmic periodic patterns
Abstract
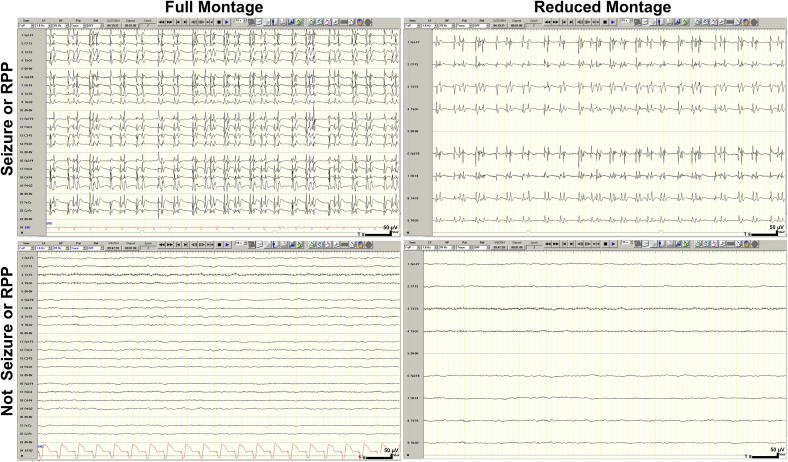
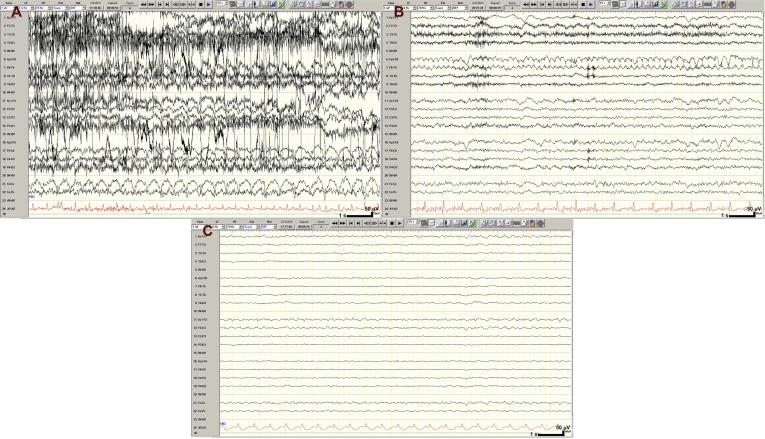
Objectives: To compare the diagnostic utility of electroencephalography (EEG) using reduced, 8-channel montage (rm-EEG) to full, 18-channel montage (fm-EEG) for detection of generalized or hemispheric seizures and rhythmic periodic patterns (RPPs) by neurologists with extensive EEG training, neurology residents with minimal EEG exposure, and medical students without EEG experience.
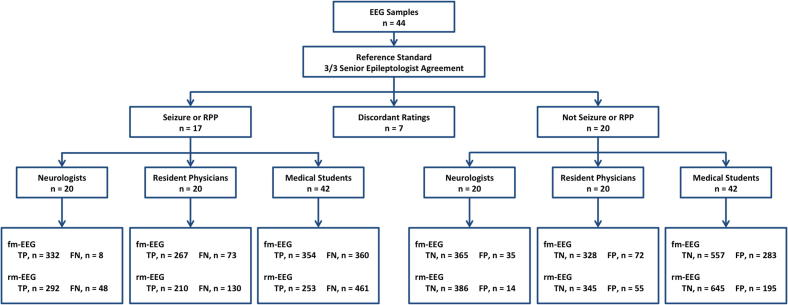
Methods: We presented EEG samples in both fm-EEG (bipolar montage) and rm-EEG (lateral leads of bipolar montage) to 20 neurologists, 20 residents, and 42 medical students. Unanimous agreement of three senior epileptologists defined samples as seizures (n = 7), RPPs (n = 10), and normal or slowing (n = 20). Differences in median accuracy, sensitivity, and specificity were assessed using Wilcoxon signed-rank tests.
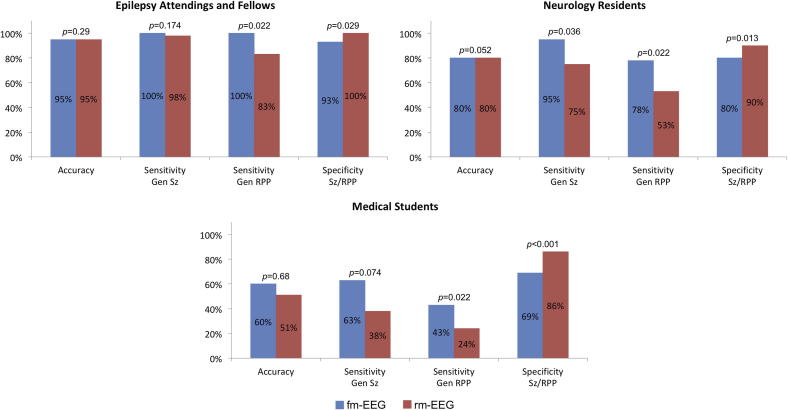
Results: Full and reduced EEG demonstrated similar accuracy when read by neurologists (fm-EEG: 95%, rm-EEG: 95%, p = 0.29), residents (fm-EEG: 80%, rm-EEG: 80%, p = 0.05), and students (fm-EEG: 60%, rm-EEG: 51%, p = 0.68). Moreover, neurologists' sensitivity for detecting seizure activity was comparable between fm-EEG (100%) and rm-EEG (98%) (p = 0.17). Furthermore, the specificity of rm-EEG for seizures and RPP (neurologists: 100%, residents: 90%, students: 86%) was significantly greater than that of fm-EEG (neurologists: 93%, p = 0.03; residents: 80%, p = 0.01; students: 69%, p < 0.001).
Conclusions: The reduction of the number of EEG channels from 18 to 8 does not compromise neurologists' sensitivity for detecting seizures that are often a core reason for performing urgent EEG. It may also increase their specificity for detecting rhythmic and periodic patterns, and thereby providing important diagnostic information to guide patient's management.
Significance: Our study is the first to document the utility of a reduced channel EEG above the hairline compared to full montage EEG in aiding medical staff with varying degrees of EEG training to detect generalized or hemispheric seizures.
Keywords: Electroencephalography; Reduced channel montage; Rhythmic and periodic patterns; Seizure detection; Sensitivity; Specificity.
Figures
References
-
- Acharya J.N., Hani A., Cheek J., Thirumala P., Tsuchida T.N. American clinical neurophysiology society guideline 2: guidelines for standard electrode position nomenclature. J. Clin. Neurophysiol. 2016;33:308–311. - PubMed
-
- Acharya J.N., Hani A.J., Thirumala P.D., Tsuchida T.N. American clinical neurophysiology society guideline 3: a proposal for standard montages to be used in clinical EEG. J. Clin. Neurophysiol. 2016;33:312–316. - PubMed
-
- Betjemann J.P., Lowenstein D.H. Status epilepticus in adults. Lancet Neurol. 2015;14:615–624. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
