

Using network analysis to localize the epileptogenic zone from invasive EEG recordings in intractable focal epilepsy
- PMID: 30215034
- PMCID: PMC6130438
- DOI: 10.1162/netn_a_00043
Using network analysis to localize the epileptogenic zone from invasive EEG recordings in intractable focal epilepsy
Abstract
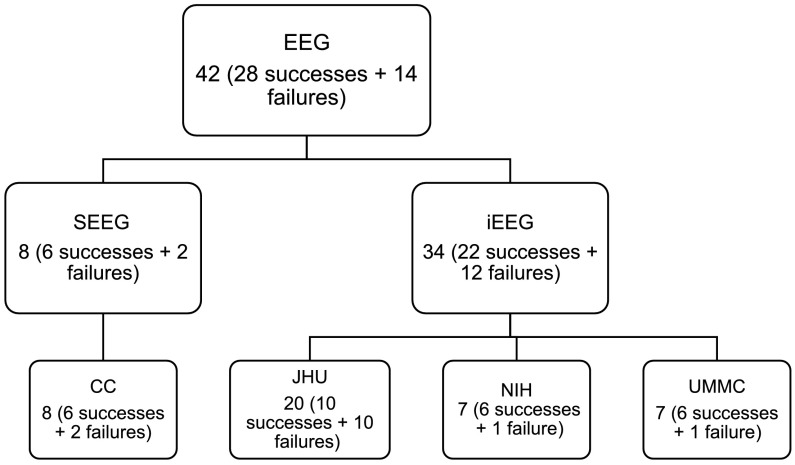
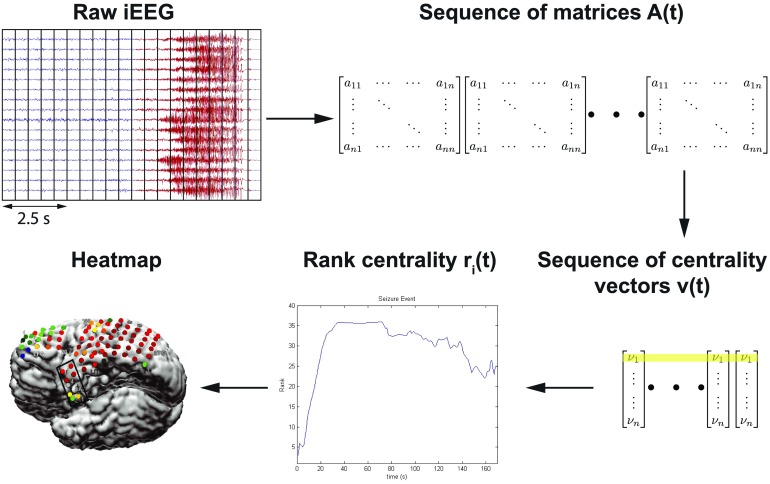
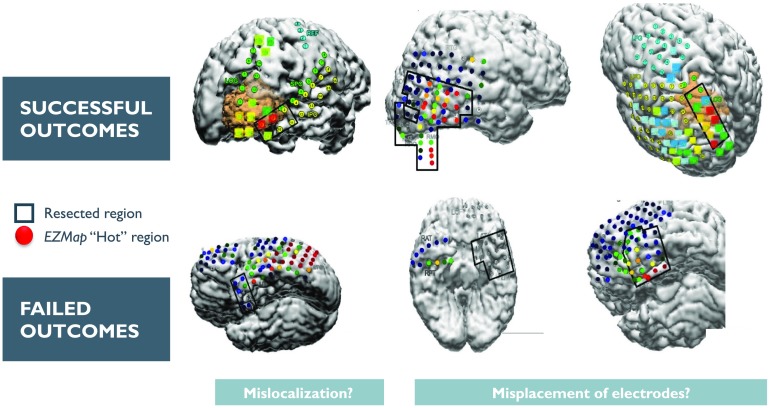
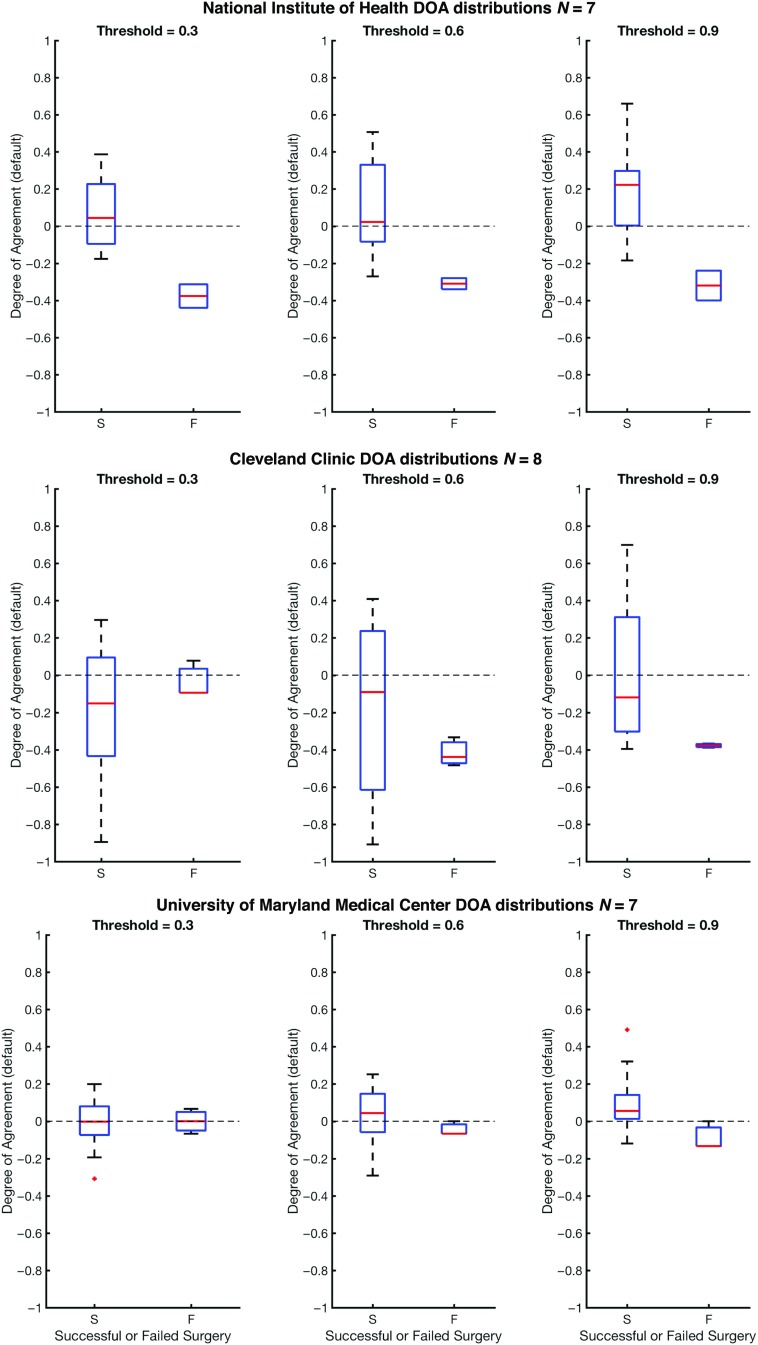
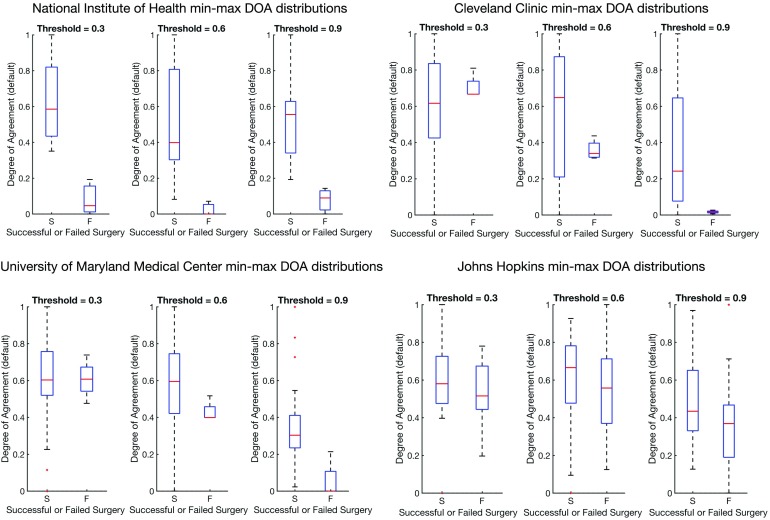
Treatment of medically intractable focal epilepsy (MIFE) by surgical resection of the epileptogenic zone (EZ) is often effective provided the EZ can be reliably identified. Even with the use of invasive recordings, the clinical differentiation between the EZ and normal brain areas can be quite challenging, mainly in patients without MRI detectable lesions. Consequently, despite relatively large brain regions being removed, surgical success rates barely reach 60-65%. Such variable and unfavorable outcomes associated with high morbidity rates are often caused by imprecise and/or inaccurate EZ localization. We developed a localization algorithm that uses network-based data analytics to process invasive EEG recordings. This network algorithm analyzes the centrality signatures of every contact electrode within the recording network and characterizes contacts into susceptible EZ based on the centrality trends over time. The algorithm was tested in a retrospective study that included 42 patients from four epilepsy centers. Our algorithm had higher agreement with EZ regions identified by clinicians for patients with successful surgical outcomes and less agreement for patients with failed outcomes. These findings suggest that network analytics and a network systems perspective of epilepsy may be useful in assisting clinicians in more accurately localizing the EZ.
Keywords: Eigenvector centrality; Focal epilepsy; Intracranial EEG; Network analysis; Seizure onset localization; Spectral models.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources