

Extent of Spinal Cord Decompression in Motor Complete (American Spinal Injury Association Impairment Scale Grades A and B) Traumatic Spinal Cord Injury Patients: Post-Operative Magnetic Resonance Imaging Analysis of Standard Operative Approaches
- PMID: 30215287
- PMCID: PMC6484360
- DOI: 10.1089/neu.2018.5834
Extent of Spinal Cord Decompression in Motor Complete (American Spinal Injury Association Impairment Scale Grades A and B) Traumatic Spinal Cord Injury Patients: Post-Operative Magnetic Resonance Imaging Analysis of Standard Operative Approaches
Abstract
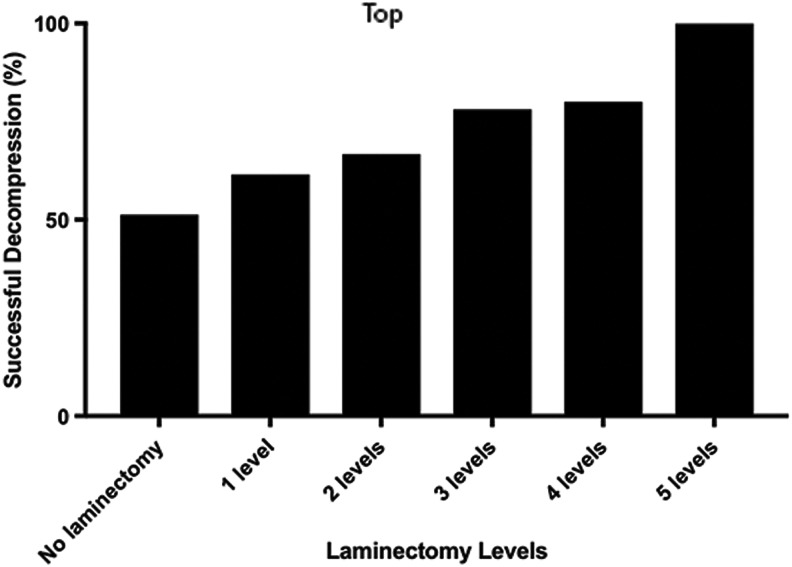
Although decompressive surgery following traumatic spinal cord injury (TSCI) is recommended, adequate surgical decompression is rarely verified via imaging. We utilized magnetic resonance imaging (MRI) to analyze the rate of spinal cord decompression after surgery. Pre-operative (within 8 h of injury) and post-operative (within 48 h of injury) MRI images of 184 motor complete patients (American Spinal Injury Association Impairment Scale [AIS] grade A = 119, AIS grade B = 65) were reviewed to verify spinal cord decompression. Decompression was defined as the presence of a patent subarachnoid space around a swollen spinal cord. Of the 184 patients, 100 (54.3%) underwent anterior cervical discectomy and fusion (ACDF), and 53 of them also underwent laminectomy. Of the 184 patients, 55 (29.9%) underwent anterior cervical corpectomy and fusion (ACCF), with (26 patients) or without (29 patients) laminectomy. Twenty-nine patients (16%) underwent stand-alone laminectomy. Decompression was verified in 121 patients (66%). The rates of decompression in patients who underwent ACDF and ACCF without laminectomy were 46.8% and 58.6%, respectively. Among these patients, performing a laminectomy increased the rate of decompression (72% and 73.1% of patients, respectively). Twenty-five of 29 (86.2%) patients who underwent a stand-alone laminectomy were found to be successfully decompressed. The rates of decompression among patients who underwent laminectomy at one, two, three, four, or five levels were 58.3%, 68%, 78%, 80%, and 100%, respectively (p < 0.001). In multi-variate logistic regression analysis, only laminectomy was significantly associated with successful decompression (odds ratio 4.85; 95% confidence interval 2.2-10.6; p < 0.001). In motor complete TSCI patients, performing a laminectomy significantly increased the rate of successful spinal cord decompression, independent of whether anterior surgery was performed.
Keywords: ASIA Impairment Scale; MRI; decompression; spinal cord injury; trauma.
Conflict of interest statement
No competing financial interests exist.
Figures



Similar articles
-
Efficacy of Ultra-Early (< 12 h), Early (12-24 h), and Late (>24-138.5 h) Surgery with Magnetic Resonance Imaging-Confirmed Decompression in American Spinal Injury Association Impairment Scale Grades A, B, and C Cervical Spinal Cord Injury.J Neurotrauma. 2020 Feb 1;37(3):448-457. doi: 10.1089/neu.2019.6606. Epub 2019 Aug 1. J Neurotrauma. 2020. PMID: 31310155 Free PMC article.
-
Intramedullary Lesion Length on Postoperative Magnetic Resonance Imaging is a Strong Predictor of ASIA Impairment Scale Grade Conversion Following Decompressive Surgery in Cervical Spinal Cord Injury.Neurosurgery. 2017 Apr 1;80(4):610-620. doi: 10.1093/neuros/nyw053. Neurosurgery. 2017. PMID: 28362913 Free PMC article.
-
Surgical Decompression of Traumatic Cervical Spinal Cord Injury: A Pilot Study Comparing Real-Time Intraoperative Ultrasound After Laminectomy With Postoperative MRI and CT Myelography.Neurosurgery. 2023 Feb 1;92(2):353-362. doi: 10.1227/neu.0000000000002207. Epub 2022 Nov 23. Neurosurgery. 2023. PMID: 36637270 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Impact of Early (<24 h) Surgical Decompression on Neurological Recovery in Thoracic Spinal Cord Injury: A Meta-Analysis.J Neurotrauma. 2019 Sep 15;36(18):2609-2617. doi: 10.1089/neu.2018.6277. Epub 2019 May 9. J Neurotrauma. 2019. PMID: 30816058
Cited by
-
The Role of Magnetic Resonance Imaging to Inform Clinical Decision-Making in Acute Spinal Cord Injury: A Systematic Review and Meta-Analysis.J Clin Med. 2021 Oct 26;10(21):4948. doi: 10.3390/jcm10214948. J Clin Med. 2021. PMID: 34768468 Free PMC article. Review.
-
Intractable postural hypotension resulting from cervical pseudomeningocele after a posterior cervical spinal surgery: a case report.Spinal Cord Ser Cases. 2023 Apr 7;9(1):14. doi: 10.1038/s41394-023-00572-8. Spinal Cord Ser Cases. 2023. PMID: 37029124 Free PMC article.
-
Mechanisms of Traumatic Spinal Cord Injury AIS Grade Conversion.Neurotrauma Rep. 2025 Jun 16;6(1):506-524. doi: 10.1089/neur.2025.0035. eCollection 2025. Neurotrauma Rep. 2025. PMID: 40630651 Free PMC article. Review.
-
Under pressure - A historical vignette on surgical timing in traumatic spinal cord injury.Brain Spine. 2024 May 3;4:102825. doi: 10.1016/j.bas.2024.102825. eCollection 2024. Brain Spine. 2024. PMID: 38756860 Free PMC article. Review.
-
Synchronized and integrated prehospital treatment for acute cervical spinal cord injury.Am J Transl Res. 2021 Jun 15;13(6):7008-7014. eCollection 2021. Am J Transl Res. 2021. PMID: 34306456 Free PMC article.
References
-
- Fehlings M.G. (2009). The impact of continued cord compression following traumatic spinal cord injury. J. Neurosurg. Spine 11, 568–569 - PubMed
-
- Carlson G.D., Gordon C.D., Oliff H.S., Pillai J.J., and Lamanna J.C. (2003). Sustained spinal cord compression: part I: time-dependent effect on long-term pathophysiology. J. Bone Jt. Surg. Am. 85-A, 86–94 - PubMed
-
- Kobrine A.I., Evans D.E., and Rizzoli H. (1978). Correlation of spinal cord blood flow and function in experimental compression. Surg. Neurol. 10, 54–59 - PubMed
-
- Kobrine A.I., Evans D.E., and V. R.H. (1979). Experimental acute balloon compression of the spinal cord. Factors affecting disappearance and return of the spinal evoked response. J. Neurosurg. 51, 841–845 - PubMed
-
- Tarlov I.M. and Herz E. (1954). Spinal cord compression studies. IV. Outlook with complete paralysis in man. AMA Arch. Neurol. Psychiatry 72, 43–59 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical