

Insulin-like Growth Factor-I Receptor and Thyroid-Associated Ophthalmopathy
- PMID: 30215690
- PMCID: PMC6338478
- DOI: 10.1210/er.2018-00066
Insulin-like Growth Factor-I Receptor and Thyroid-Associated Ophthalmopathy
Abstract
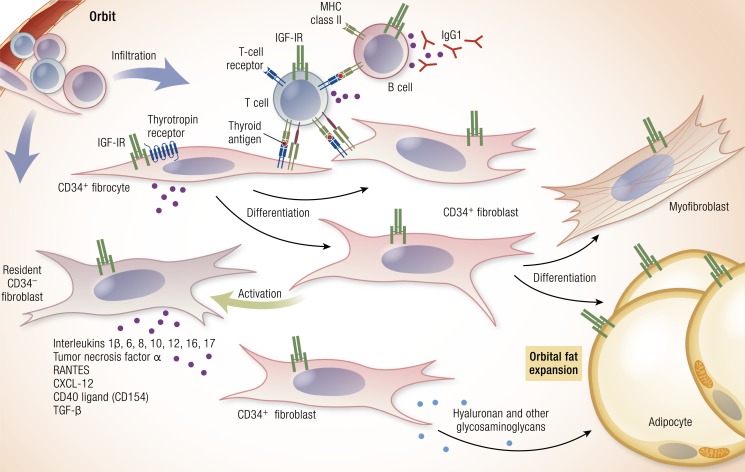
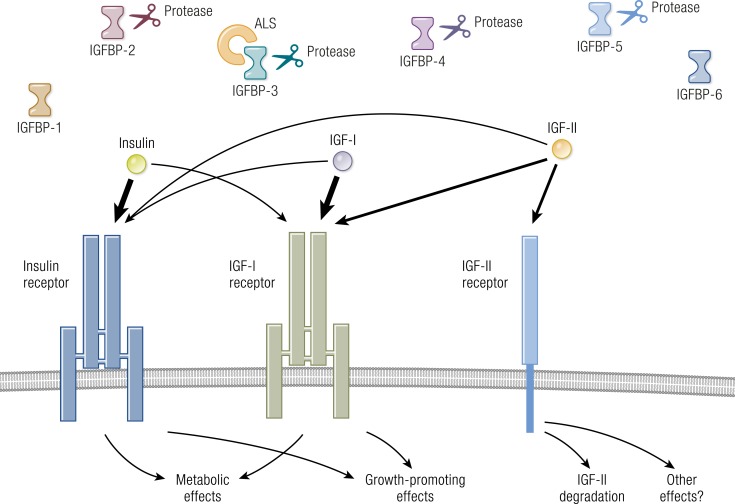
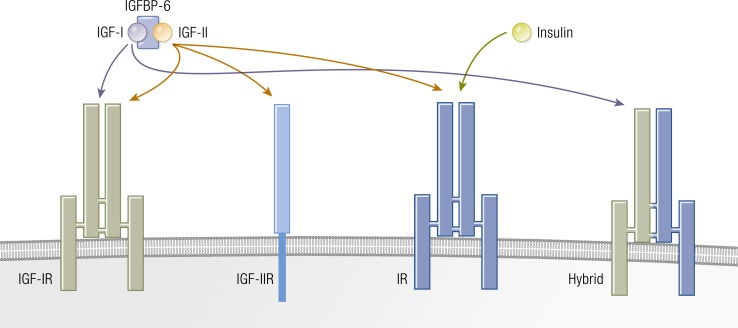
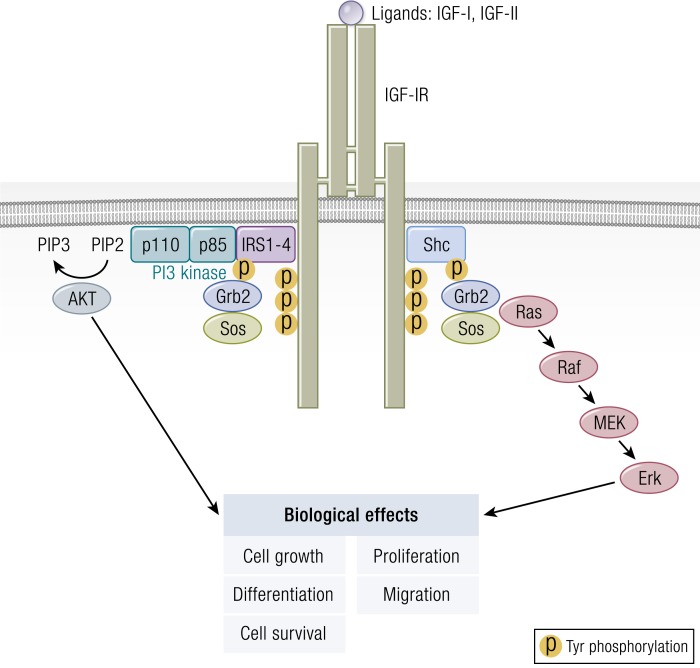
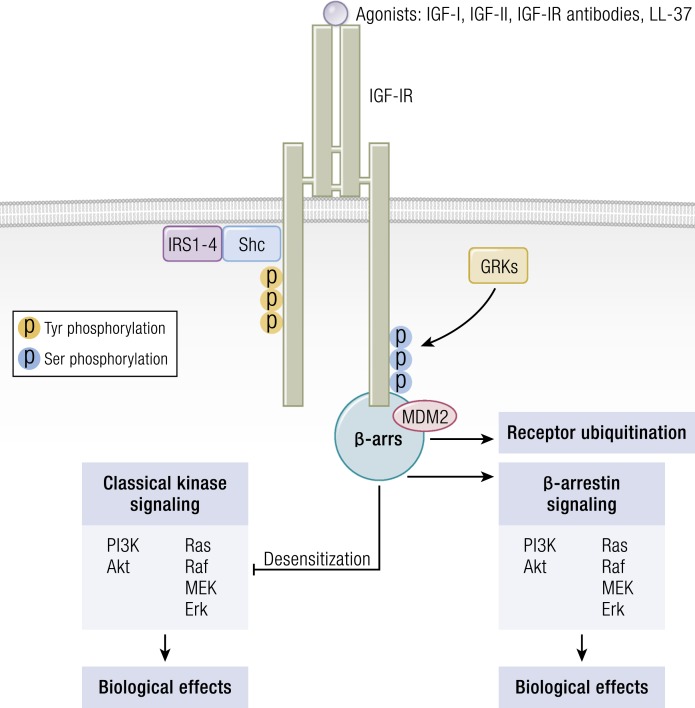
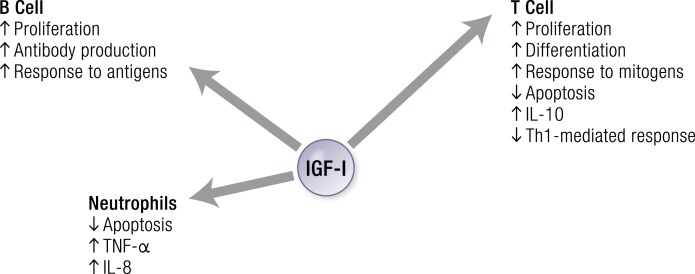
Thyroid-associated ophthalmopathy (TAO) is a complex disease process presumed to emerge from autoimmunity occurring in the thyroid gland, most frequently in Graves disease (GD). It is disfiguring and potentially blinding, culminating in orbital tissue remodeling and disruption of function of structures adjacent to the eye. There are currently no medical therapies proven capable of altering the clinical outcome of TAO in randomized, placebo-controlled multicenter trials. The orbital fibroblast represents the central target for immune reactivity. Recent identification of fibroblasts that putatively originate in the bone marrow as monocyte progenitors provides a plausible explanation for why antigens, the expressions of which were once considered restricted to the thyroid, are detected in the TAO orbit. These cells, known as fibrocytes, express relatively high levels of functional TSH receptor (TSHR) through which they can be activated by TSH and the GD-specific pathogenic antibodies that underpin thyroid overactivity. Fibrocytes also express insulin-like growth factor I receptor (IGF-IR) with which TSHR forms a physical and functional signaling complex. Notably, inhibition of IGF-IR activity results in the attenuation of signaling initiated at either receptor. Some studies suggest that IGF-IR-activating antibodies are generated in GD, whereas others refute this concept. These observations served as the rationale for implementing a recently completed therapeutic trial of teprotumumab, a monoclonal inhibitory antibody targeting IGF-IR in TAO. Results of that trial in active, moderate to severe disease revealed dramatic and rapid reductions in disease activity and severity. The targeting of IGF-IR with specific biologic agents may represent a paradigm shift in the therapy of TAO.
Figures


References
-
- Smith TJ, Hegedüs L. Graves’ disease. N Engl J Med. 2016;375(16):1552–1565. - PubMed
-
- Nordyke RA, Gilbert FI Jr, Harada AS. Graves’ disease. Influence of age on clinical findings. Arch Intern Med. 1988;148(3):626–631. - PubMed
-
- Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, Perros P, Salvi M, Wiersinga WM; European Group on Graves’ Orbitopathy (EUGOGO) . The 2016 European Thyroid Association/European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy. Eur Thyroid J. 2016;5(1):9–26. - PMC - PubMed
-
- Putta-Manohar S, Perros P. Epidemiology of Graves’ orbitopathy. Pediatr Endocrinol Rev. 2010;7(Suppl 2):182–185. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
