

Prognosticating Outcomes in Interstitial Lung Disease by Mediastinal Lymph Node Assessment. An Observational Cohort Study with Independent Validation
- PMID: 30216085
- PMCID: PMC6423102
- DOI: 10.1164/rccm.201804-0761OC
Prognosticating Outcomes in Interstitial Lung Disease by Mediastinal Lymph Node Assessment. An Observational Cohort Study with Independent Validation
Abstract
Rationale: Mediastinal lymph node (MLN) enlargement on chest computed tomography (CT) is prevalent in patients with interstitial lung disease (ILD) and may reflect immunologic activation and subsequent cytokine-mediated immune cell trafficking.
Objectives: We aimed to determine whether MLN enlargement on chest CT predicts clinical outcomes and circulating cytokine levels in ILD.
Methods: MLN measurements were obtained from chest CT scans of patients with ILD at baseline evaluation over a 10-year period. Patients with sarcoidosis and drug toxicity-related ILD were excluded. MLN diameter and location were assessed. Plasma cytokine levels were analyzed in a subset of patients. The primary outcome was transplant-free survival (TFS). Secondary outcomes included all-cause and respiratory hospitalizations, lung function, and plasma cytokine concentrations. Cox regression was used to assess mortality risk. Outcomes were assessed in three independent ILD cohorts.
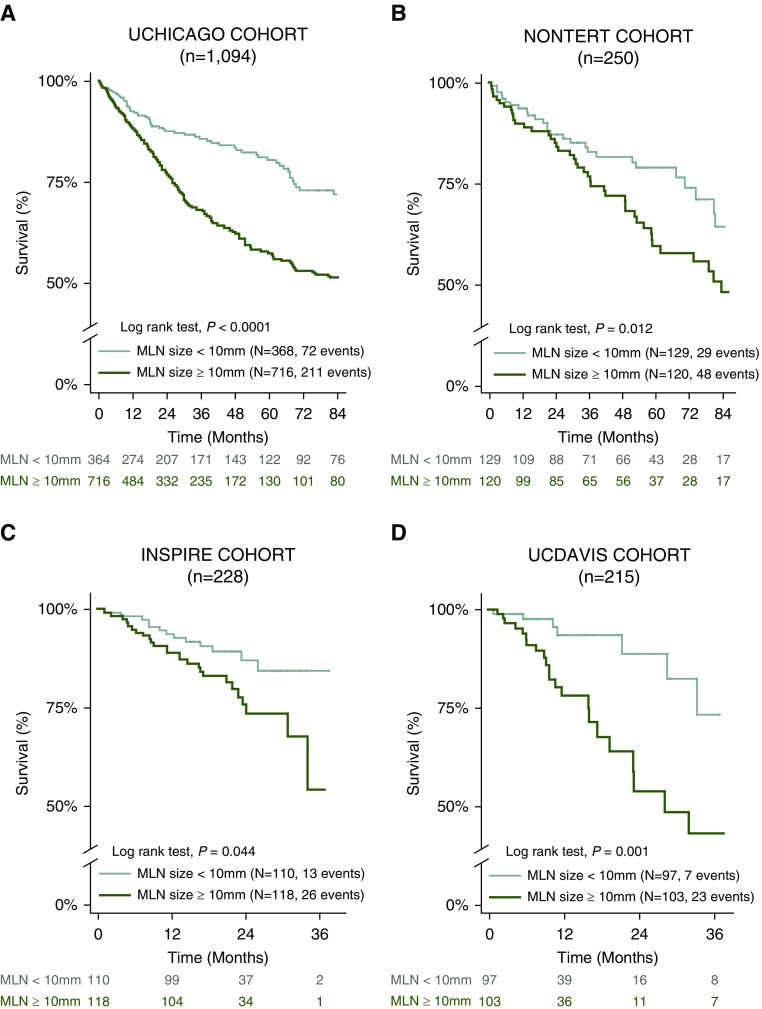
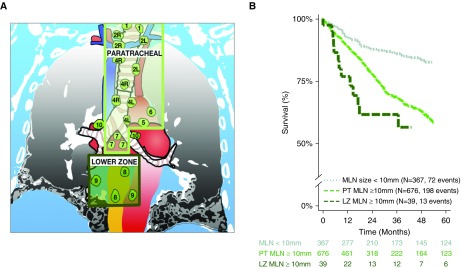
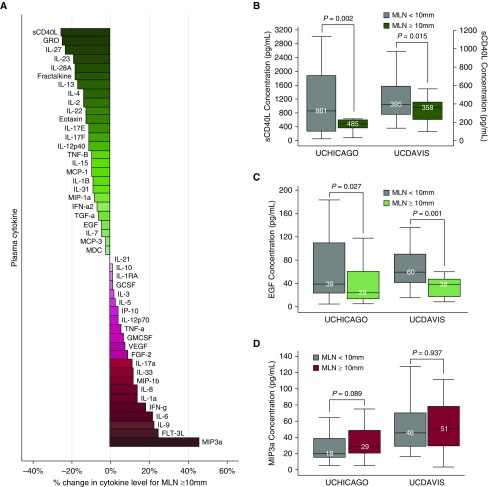
Measurements and main results: Chest CT scans were assessed in 1,094 patients (mean age, 64 yr; 52% male). MLN enlargement (≥10 mm) was present in 66% (n = 726) and strongly predicted TFS (hazard ratio [HR], 1.53; 95% confidence interval [CI], 1.12-2.10; P = 0.008) and risk of all-cause and respiratory hospitalizations (internal rate of return [IRR], 1.52; 95% CI, 1.17-1.98; P = 0.002; and IRR, 1.71; 95% CI, 1.15-2.53; P = 0.008, respectively) when compared with subjects with MLN <10 mm. Patients with MLN enlargement had lower lung function and decreased plasma concentrations of soluble CD40L (376 pg/ml vs. 505 pg/ml, P = 0.001) compared with those without MLN enlargement. Plasma IL-10 concentration >45 pg/ml predicted mortality (HR, 4.21; 95% CI, 1.21-14.68; P = 0.024). Independent analysis of external datasets confirmed these findings.
Conclusions: MLN enlargement predicts TFS and hospitalization risk in ILD and is associated with decreased levels of a key circulating cytokine, soluble CD40L. Incorporating MLN and cytokine findings into current prediction models might improve ILD prognostication.
Keywords: interstitial lung disease; mediastinal lymph nodes; mortality; pulmonary fibrosis.
Figures
Comment in
-
Mediastinal Lymphadenopathy in Interstitial Lung Disease. Time to Be Counted.Am J Respir Crit Care Med. 2019 Mar 15;199(6):685-687. doi: 10.1164/rccm.201810-1892ED. Am J Respir Crit Care Med. 2019. PMID: 30335464 Free PMC article. No abstract available.
-
Reply to Lescoat et al. and to Khamis et al.Am J Respir Crit Care Med. 2019 Apr 15;199(8):1041-1042. doi: 10.1164/rccm.201811-2208LE. Am J Respir Crit Care Med. 2019. PMID: 30653922 Free PMC article. No abstract available.
-
Interstitial Lung Disease and Mediastinal Lymph Nodes: A Computed Tomography-based Biomarker beyond Nosological and Etiological Borders?Am J Respir Crit Care Med. 2019 Apr 15;199(8):1038-1040. doi: 10.1164/rccm.201811-2123LE. Am J Respir Crit Care Med. 2019. PMID: 30653924 Free PMC article. No abstract available.
-
Prognostic Impact of Mediastinal Lymph Nodes in Interstitial Lung Diseases: Is Environmental Exposure the Offender?Am J Respir Crit Care Med. 2019 Apr 15;199(8):1040-1041. doi: 10.1164/rccm.201811-2209LE. Am J Respir Crit Care Med. 2019. PMID: 30653925 Free PMC article. No abstract available.
References
-
- Raghu G. Epidemiology, survival, incidence and prevalence of idiopathic pulmonary fibrosis in the USA and Canada. Eur Respir J. 2017;49:1602384. - PubMed
-
- Raghu G, Chen SY, Hou Q, Yeh WS, Collard HR. Incidence and prevalence of idiopathic pulmonary fibrosis in US adults 18–64 years old. Eur Respir J. 2016;48:179–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
