

Severely malnourished children with a low weight-for-height have similar mortality to those with a low mid-upper-arm-circumference: II. Systematic literature review and meta-analysis
- PMID: 30217196
- PMCID: PMC6138903
- DOI: 10.1186/s12937-018-0383-5
Severely malnourished children with a low weight-for-height have similar mortality to those with a low mid-upper-arm-circumference: II. Systematic literature review and meta-analysis
Abstract
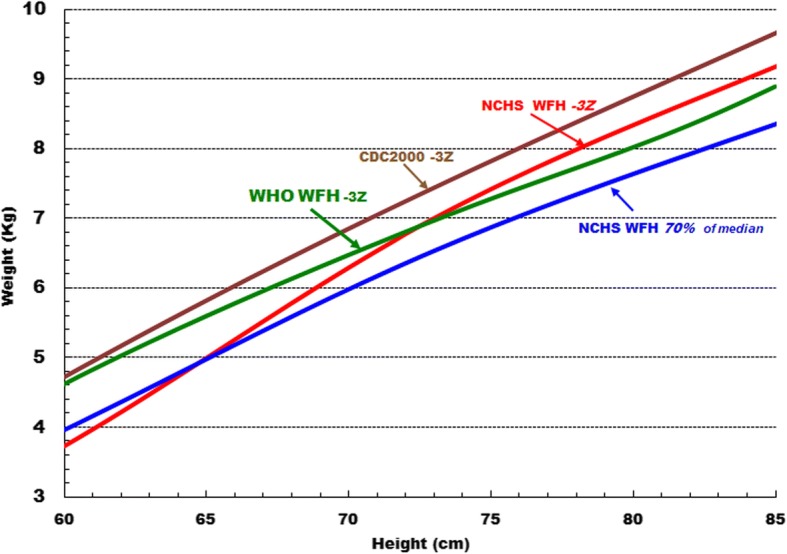
Background: The WHO recommended criteria for diagnosis of sever acute malnutrition (SAM) are weight-for-height/length Z-score (WHZ) of <- 3Z of the WHO2006 standards, a mid-upper-arm circumference (MUAC) of < 115 mm, nutritional oedema or any combination of these parameters. A move to eliminate WHZ as a diagnostic criterion has been made on the assertion that children with a low WHZ are healthy, that MUAC is a "superior" prognostic indicator of mortality and that adding WHZ to the assessment does not improve the prediction of death. Our objective was to examine the literature comparing the risk of death of SAM children admitted by WHZ or MUAC criteria.
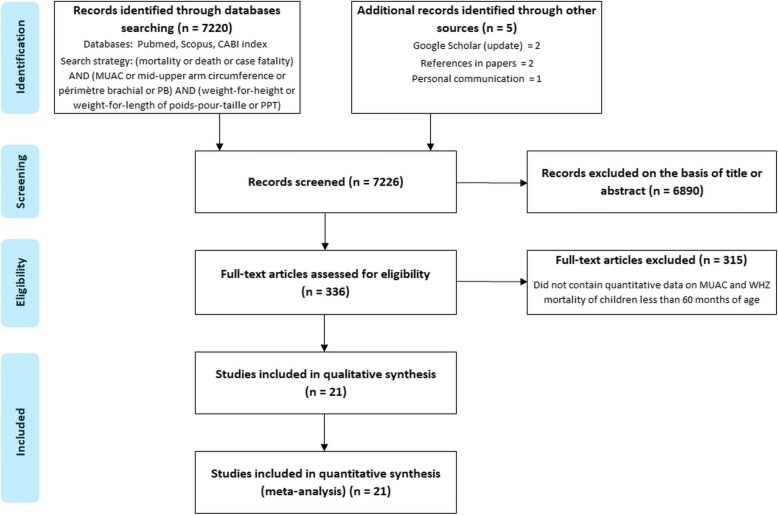
Methods: We conducted a systematic search for reports which examined the relationship of WHZ and MUAC to mortality for children less than 60 months. The WHZ, MUAC, outcome and programmatic variables were abstracted from the reports and examined. Individual study's case fatality rates were compared by chi-squared analysis and random effects meta-analyses for combined data.
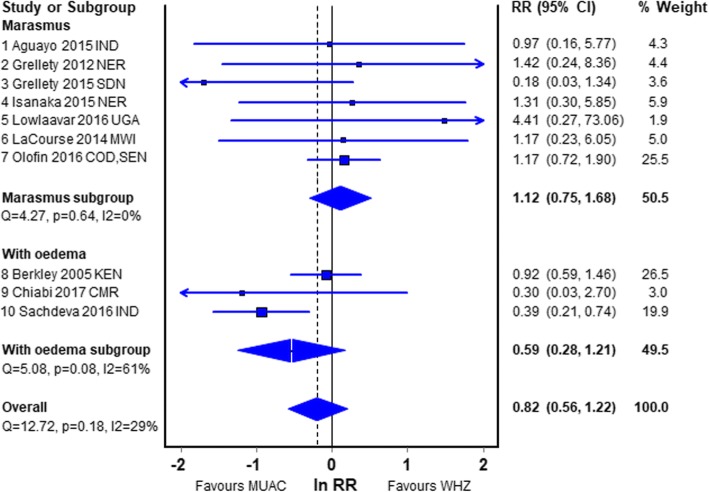
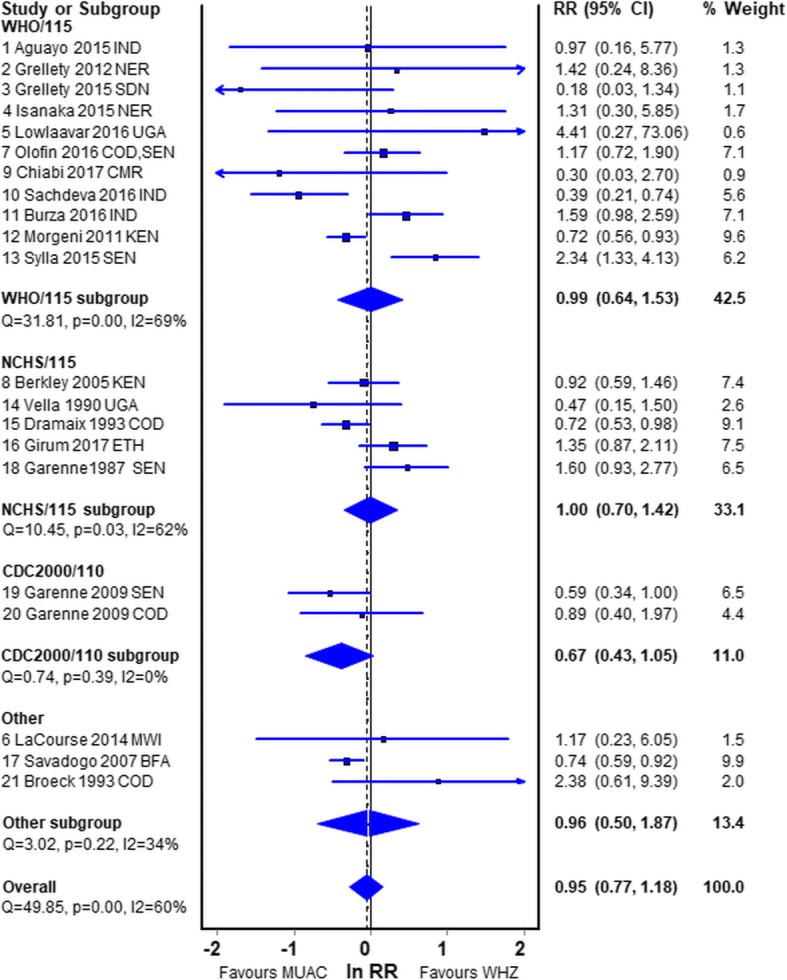
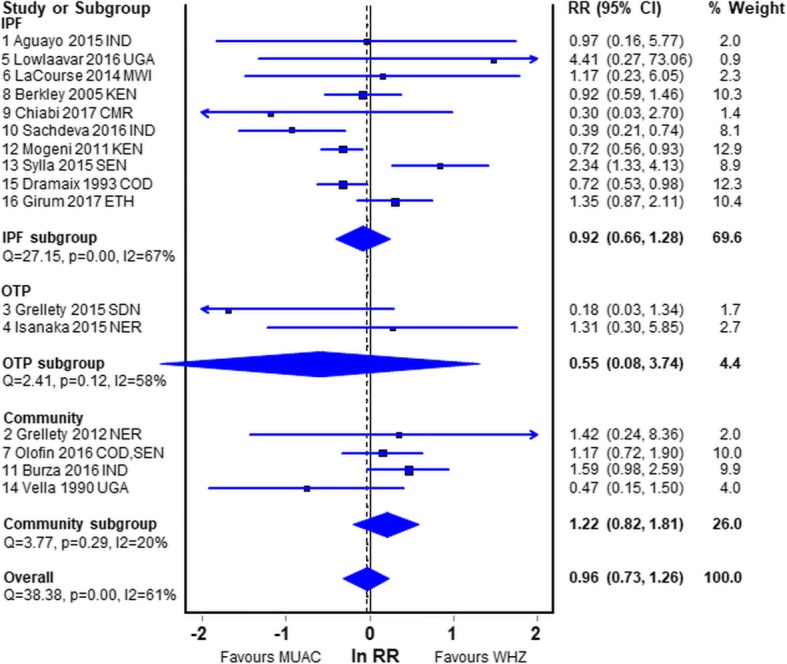
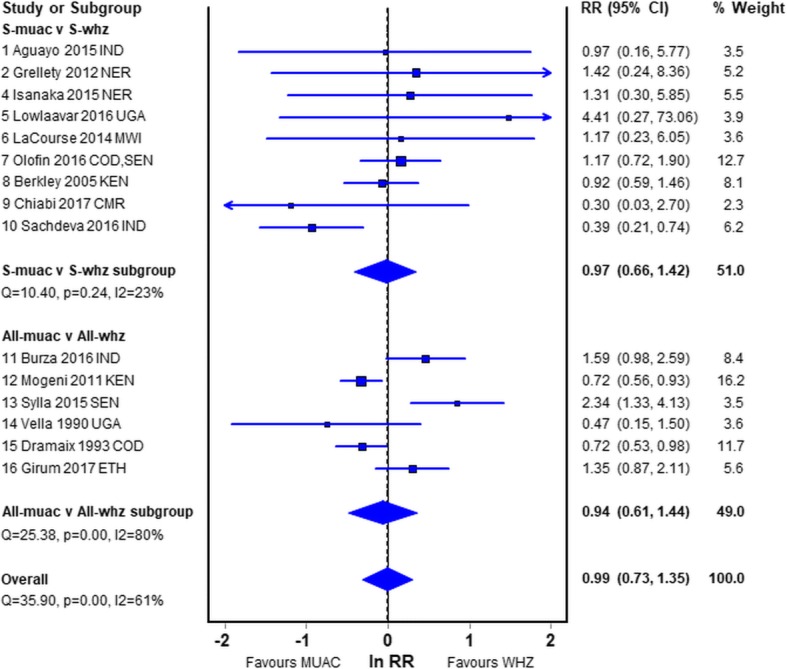
Results: Twenty-one datasets were reviewed. All the patient studies had an ascertainment bias. Most were inadequate because they had insufficient deaths, used obsolete standards, combined oedematous and non-oedematous subjects, did not report the proportion of children with both deficits or the deaths occurred remotely after anthropometry. The meta-analyses showed that the mortality risks for children who have SAM by MUAC < 115 mm only and those with SAM by WHZ < -3Z only are not different.
Conclusions: As the diagnostic criteria identify different children, this analysis does not support the abandonment of WHZ as an important independent diagnostic criterion for the diagnosis of SAM. Failure to identify such children will result in their being denied treatment and unnecessary deaths from SAM.
Keywords: Acute malnutrition; Case fatality rate; Child; Diagnosis; Human; Kwashiorkor; MUAC; Meta-analysis; Mid-upper-arm circumference; Mortality; Nutrition; Oedema; SAM; Severe acute malnutrition; Simpson’s paradox; Systematic review; WHZ; Wasting; Weight-for-height.
Conflict of interest statement
Ethics approval and consent to participate
This is a secondary analysis of anonymous data which is in the public domain. As no individual, location or administrative district could be identified no formal ethical clearance was required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- John C, Ocheke IE, Diala U, Adah RO, Envuladu EA. Does mid upper arm circumference identify all acute malnourished 6-59 month old children, in field and clinical settings in Nigeria? S Afr J Clin Nutr. 2016;1–5. http://www.tandfonline.com/doi/abs/10.1080/16070658.2016.1255486. - DOI
-
- Manyike PC, Chinawa JM, Ubesie A, Obu HA, Odetunde OI, Chinawa AT. Prevalence of malnutrition among pre-school children in, South-east Nigeria. Italian J Pediatrics. 2014;40:75. https://ijponline.biomedcentral.com/articles/10.1186/s13052-014-0075-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
