

Estimating abortion incidence among adolescents and differences in postabortion care by age: a cross-sectional study of postabortion care patients in Uganda
- PMID: 30217474
- PMCID: PMC6219390
- DOI: 10.1016/j.contraception.2018.07.135
Estimating abortion incidence among adolescents and differences in postabortion care by age: a cross-sectional study of postabortion care patients in Uganda
Abstract
Objectives: To provide the first estimate of adolescents' abortion incidence in Uganda and to assess differences in the abortion experiences and morbidities of adolescent and nonadolescent postabortion care (PAC) patients.
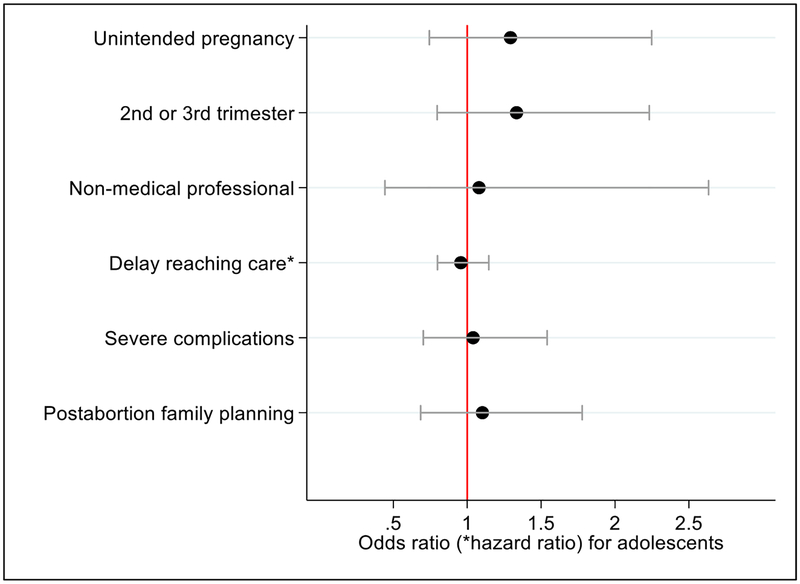
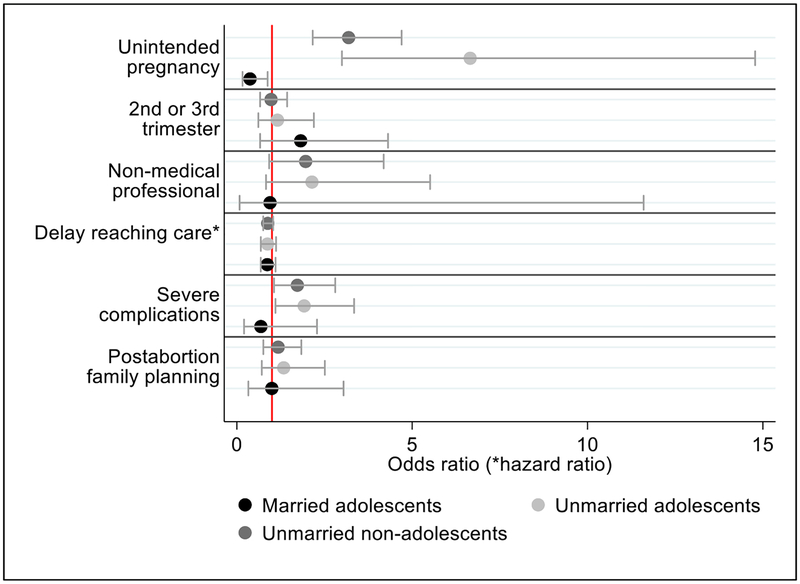
Study design: We used the age-specific Abortion Incidence Complications Method, drawing from three surveys conducted in Uganda in 2013: a nationally representative Health Facilities Survey (n=418), a Health Professionals Survey (n=147) and a Prospective Morbidity Survey of PAC patients (n=2169). Multivariable logistic and Cox proportional hazard models were used to compare adolescent and nonadolescent PAC patients on dimensions including pregnancy intention, gestational age, abortion safety, delays to care, severity of complications and receipt of postabortion family planning. We included an interaction term between adolescents and marital status to assess heterogeneity among adolescents.
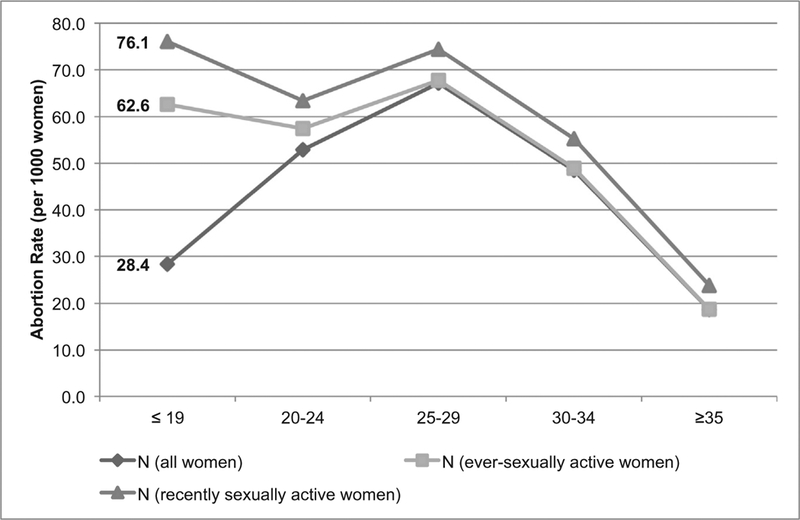
Results: Adolescent women have the lowest abortion rate among women less than 35 years of age (28.4 abortions per 1000 women 15-19) but the highest rate among recently sexually active women (76.1 abortions per 1000 women 15-19). We do not find that adolescents face greater disadvantages in their abortion care experiences as compared to older women. However, unmarried PAC patients, both adolescent and nonadolescent, have higher odds of experiencing severe complications than nonadolescent married women.
Conclusions: The high abortion rate among sexually active adolescents highlights the critical need to improve adolescent family planning in Uganda. Interventions to prevent unintended pregnancy and to reduce unsafe abortion may be particularly important for unmarried adolescents. Rather than treating adolescents as a homogenous group, we need to understand how marriage and other social factors shape reproductive health outcomes.
Implications: This paper provides the first estimate of the adolescent abortion rate in Uganda. Studies of adolescent abortion and reproductive health must account for sexual activity and marital status. Further, interventions to address unintended pregnancy and unsafe abortion among unmarried women of all ages in Africa should be a priority.
Keywords: Abortion complications; Adolescent; Family planning; Induced abortion; Unintended pregnancy.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Uganda Bureau of Statistics (UBOS), ICF. Uganda demographic and health survey 2016. Kampala, Uganda and Rockville, Maryland, USA: UBOS and ICF; 2018.
-
- Kaye DK, Mirembe F, Bantebya G, Johansson A, Ekstrom AM. Reasons, methods used and decision-making for pregnancy termination among adolescents and older women in Mulago hospital, Uganda. East Afr Med J 2005;82:579–85. - PubMed
-
- Olukoya AA, Kaya A, Ferguson BJ, AbouZahr C. Unsafe abortion in adolescents. Int J Gynaecol Obstet 2001;75:137–47. - PubMed
-
- Reproductive Health Division, Department of Community Health, Ministry of Health, Republic of Uganda. The national policy guidelines and service standards for sexual and reproductive health and rights. Kampala, Uganda: Ministry of Health, Uganda; 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
