

Management of oesophageal intramucosal carcinoma
- PMID: 30217797
- PMCID: PMC6144262
- DOI: 10.1136/bcr-2018-224893
Management of oesophageal intramucosal carcinoma
Abstract
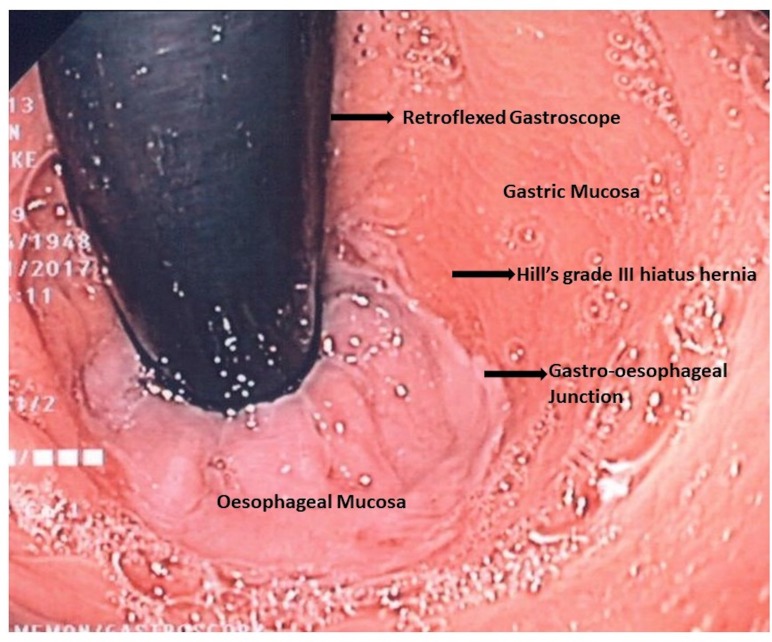
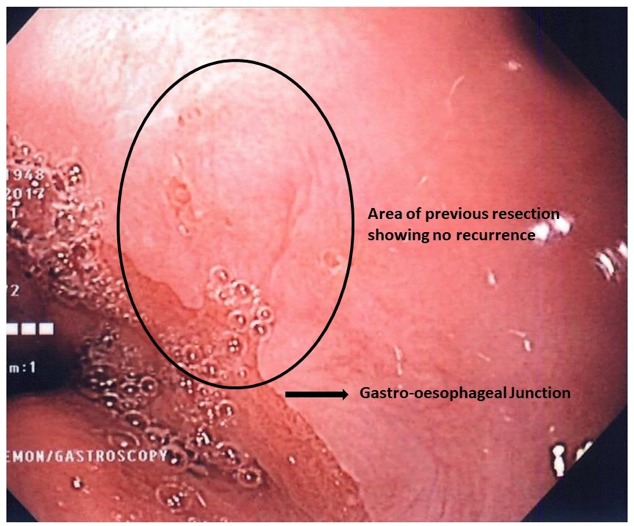
We present an interesting case of an intramucosal carcinoma (IMC) in the setting of Barrett's oesophagus in a 66-year-old woman. Her clinical course highlights the shifting paradigm in the approach to management of Barrett's oesophagus and IMC. With innovation in imaging and endoscopic treatment modalities, patients are detected earlier and managed prior to development of malignancy. The patient was treated with endoscopic modalities, and after 3 years' follow-up, she remains recurrence free.
Keywords: gastric cancer; gastrointestinal surgery; general surgery.
© BMJ Publishing Group Limited 2018. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical