

Mechanisms, biomarkers and targets for adult-onset Still's disease
- PMID: 30218025
- PMCID: PMC7097309
- DOI: 10.1038/s41584-018-0081-x
Mechanisms, biomarkers and targets for adult-onset Still's disease
Abstract
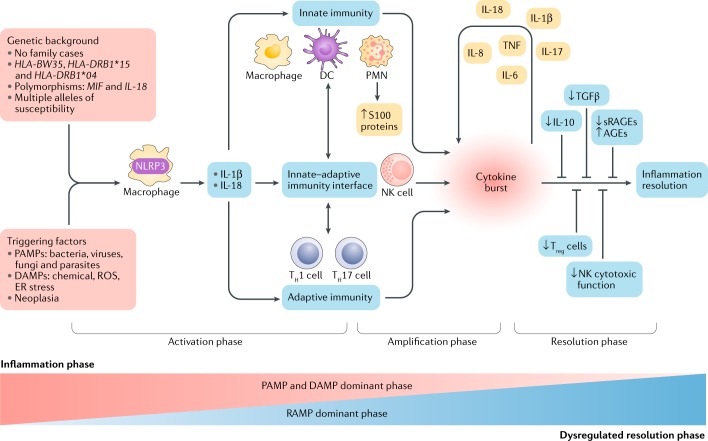
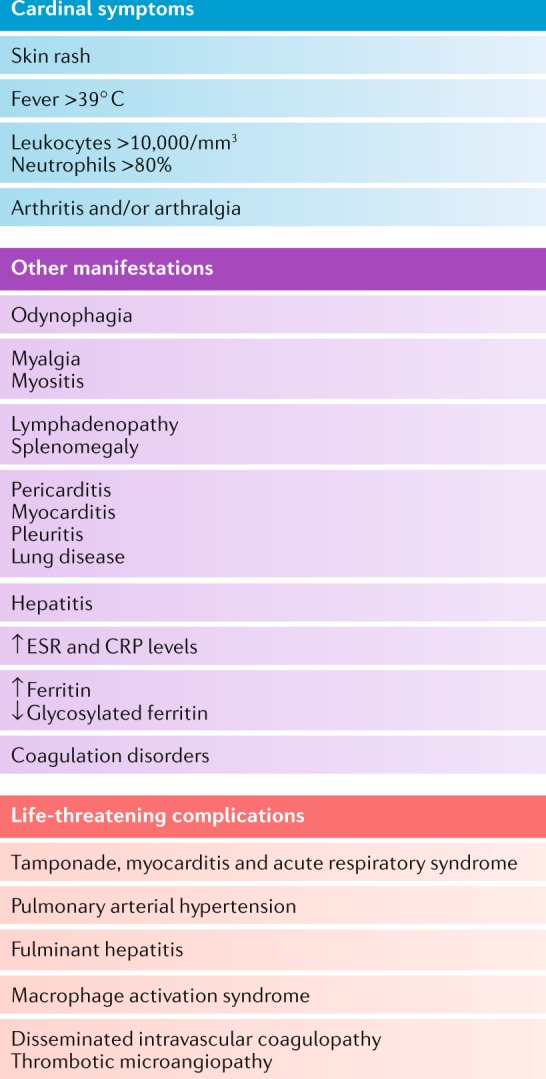
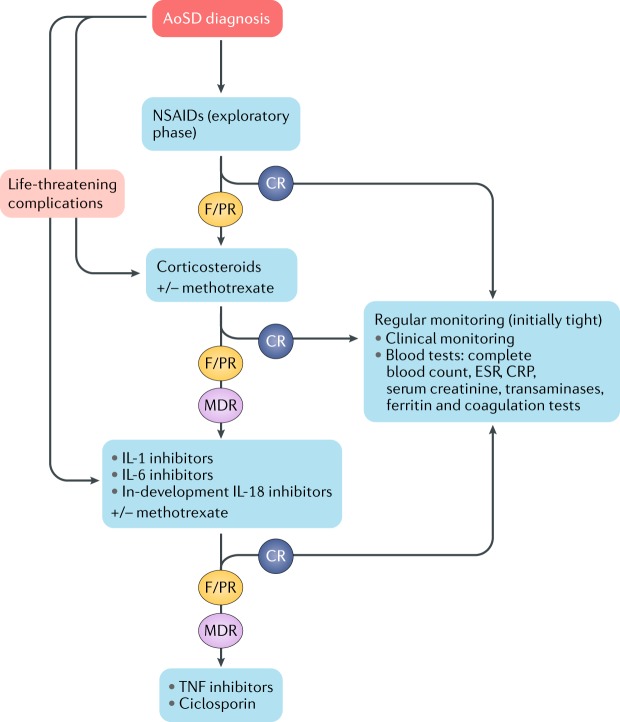
Adult-onset Still's disease (AoSD) is a rare but clinically well-known, polygenic, systemic autoinflammatory disease. Owing to its sporadic appearance in all adult age groups with potentially severe inflammatory onset accompanied by a broad spectrum of disease manifestation and complications, AoSD is an unsolved challenge for clinicians with limited therapeutic options. This Review provides a comprehensive insight into the complex and heterogeneous nature of AoSD, describing biomarkers of the disease and its progression and the cytokine signalling pathways that contribute to disease. The efficacy and safety of biologic therapeutic options are also discussed, and guidance for treatment decisions is provided. Improving the approach to AoSD in the future will require much closer cooperation between paediatric and adult rheumatologists to establish common diagnostic strategies, treatment targets and goals.
Conflict of interest statement
E.F. has received consultant fees from AbbVie, Biogen, BMS, Celgene, Janssen, Lilly, Medac, MSD, Nordic Pharma, Novartis, Pfizer, Roche, Sanofi-Aventis, Swedish Orphan Biovitrum and UCB, as well as research grants from BMS, Lilly, Novartis, Pfizer and Roche. S.M. has received consultant fees from BMS and Pfizer. B.F. has received consultant fees from AbbVie, Biogen, BMS, Celgene, Janssen, Lilly, Medac, MSD, Nordic Pharma, Novartis, Pfizer, Roche, Sanofi-Aventis, Swedish Orphan Biovitrum and UCB, as well as research grants from AbbVie, MSD and Pfizer.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
