

The clinical features, underlying immunology, and treatment of autoantibody-mediated movement disorders
- PMID: 30218501
- PMCID: PMC6221172
- DOI: 10.1002/mds.27446
The clinical features, underlying immunology, and treatment of autoantibody-mediated movement disorders
Abstract
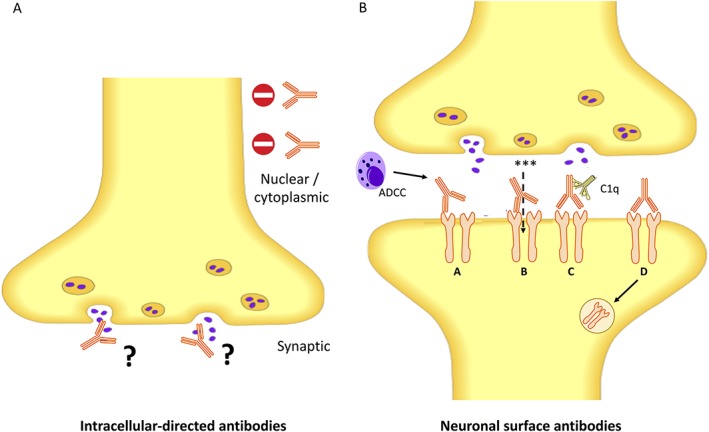
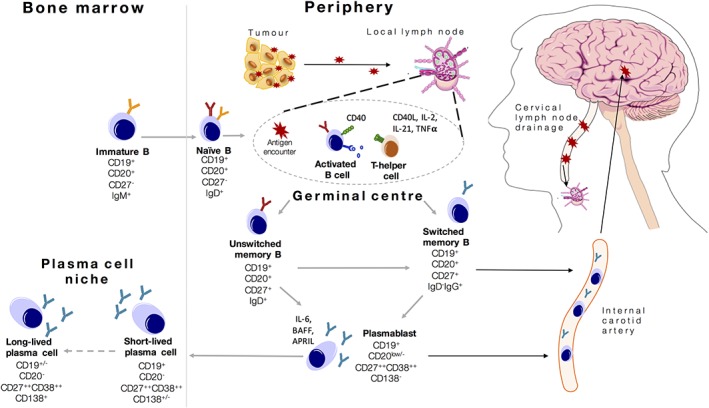
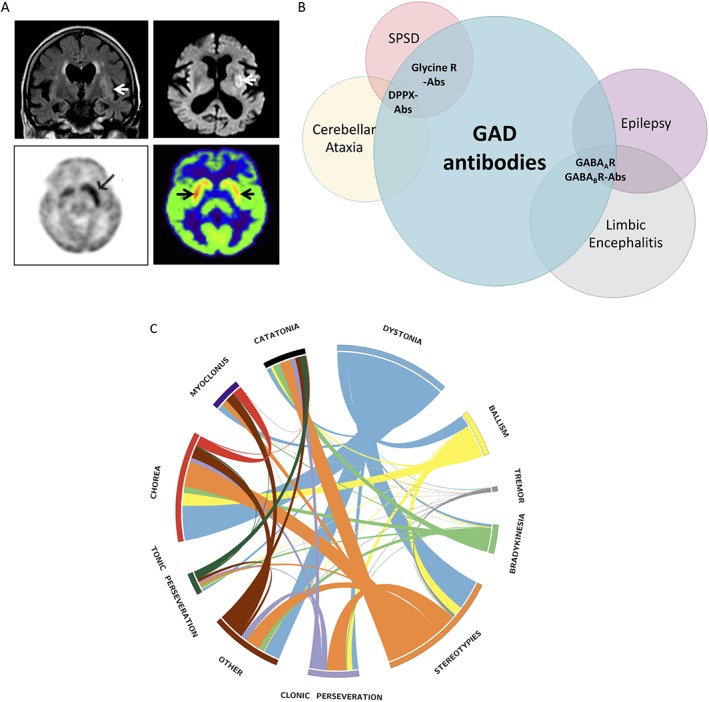
An increasing number of movement disorders are associated with autoantibodies. Many of these autoantibodies target the extracellular domain of neuronal surface proteins and associate with highly specific phenotypes, suggesting they have pathogenic potential. Below, we describe the phenotypes associated with some of these commoner autoantibody-mediated movement disorders, and outline increasingly well-established mechanisms of autoantibody pathogenicity which include antigen downregulation and complement fixation. Despite these advances, and the increasingly robust evidence for improved clinical outcomes with early escalation of immunotherapies, the underlying cellular immunology of these conditions has received little attention. Therefore, here, we outline the likely roles of T cells and B cells in the generation of autoantibodies, and reflect on how these may guide both current immunotherapy regimes and our future understanding of precision medicine in the field. In addition, we summarise potential mechanisms by which these peripherally-driven immune responses may reach the central nervous system. We integrate this with the immunologically-relevant clinical observations of preceding infections, tumours and human leucocyte antigen-associations to provide an overview of the therapeutically-relevant underlying adaptive immunology in the autoantibody-mediated movement disorders. © 2018 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: Neuroimmunology; autoantibody; autoimmune encephalitis; immunology; stiff person syndrome.
© 2018 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Figures
References
-
- Baizabal‐Carvallo JF, Jankovic J. Movement disorders in autoimmune diseases. Mov Disord 2012;27(8):935‐946. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
