

Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: a systematic review and meta-analysis
- PMID: 30219047
- PMCID: PMC6139159
- DOI: 10.1186/s12890-018-0718-1
Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: a systematic review and meta-analysis
Abstract
Background: Pulmonary rehabilitation (PR), delivered as a supervised multidisciplinary program including exercise training, is one of the cornerstones in the chronic obstructive pulmonary disease (COPD) management. We performed a systematic review and meta-analysis to assess the effect on mortality of a supervised early PR program, initiated during or within 4 weeks after hospitalization with an acute exacerbation of COPD compared with usual post-exacerbation care or no PR program. Secondary outcomes were days in hospital, COPD related readmissions, health-related quality of life (HRQoL), exercise capacity (walking distance), activities of daily living (ADL), fall risk and drop-out rate.
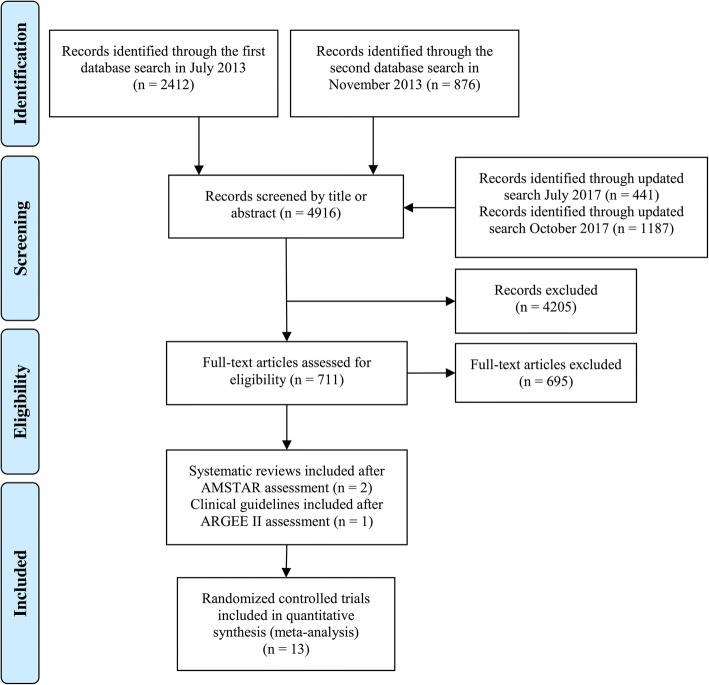
Methods: We identified randomized trials through a systematic search using MEDLINE, EMBASE and Cocharne Library and other sources through October 2017. Risk of bias was assessed regarding randomization, allocation sequence concealment, blinding, incomplete outcome data, selective outcome reporting, and other biases using the Cochrane Risk of Bias tool.
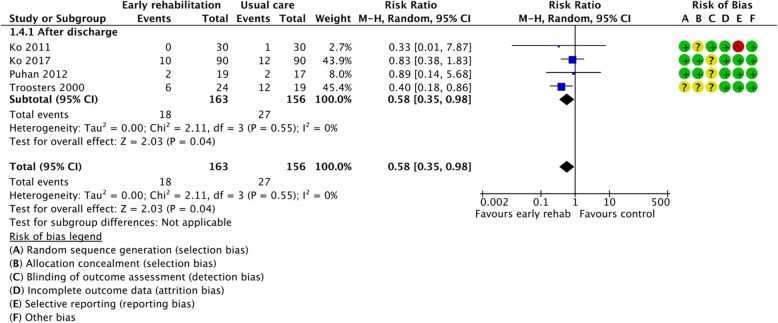
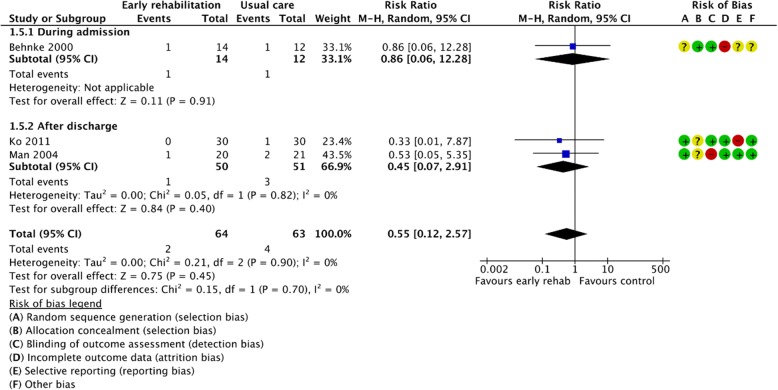
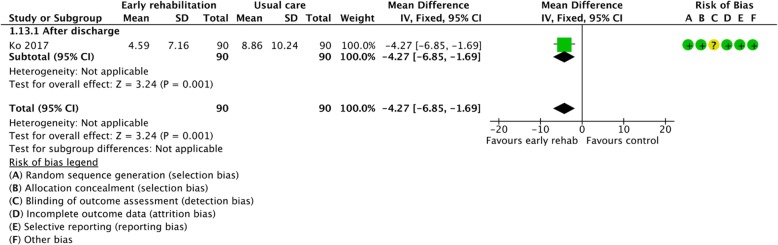
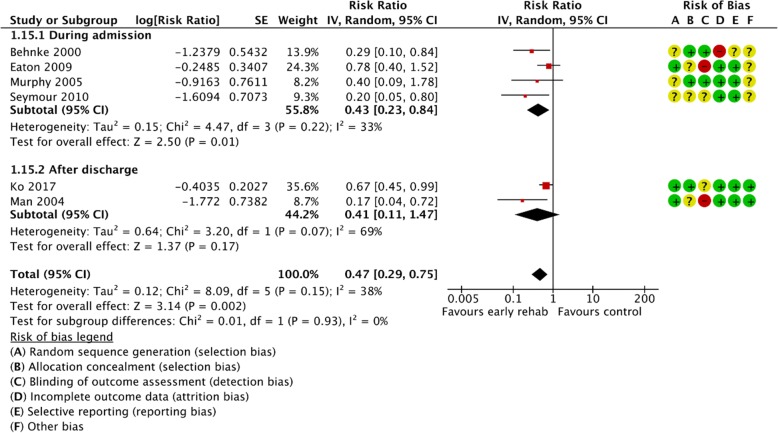
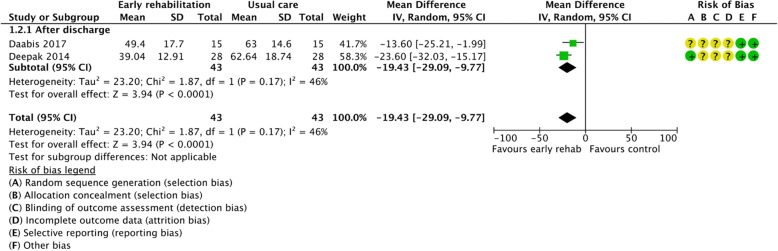
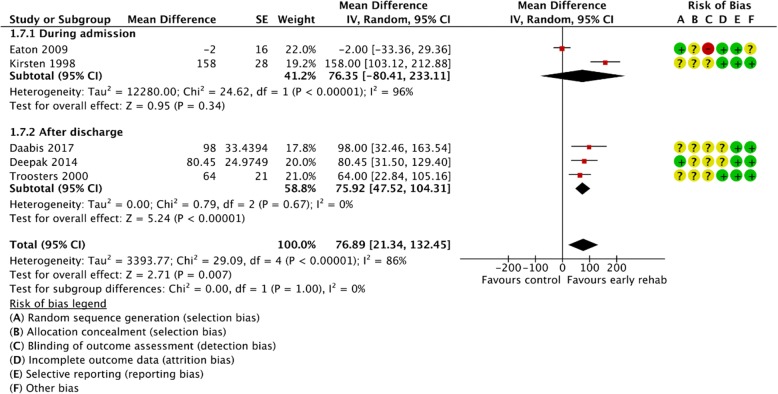
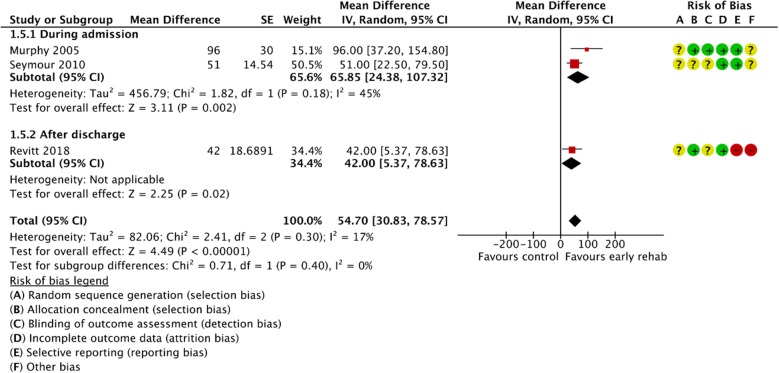
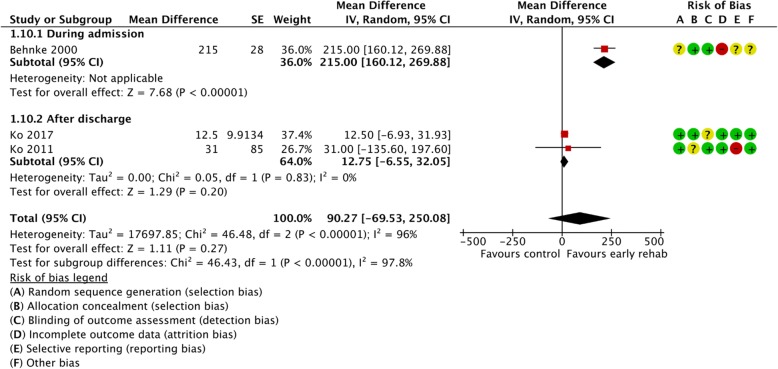
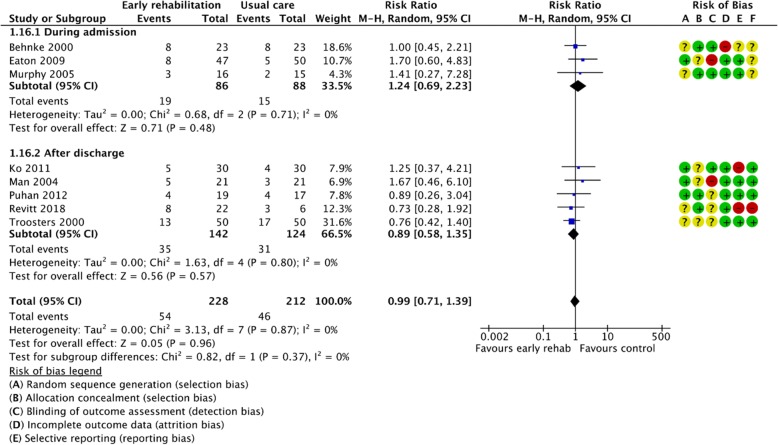
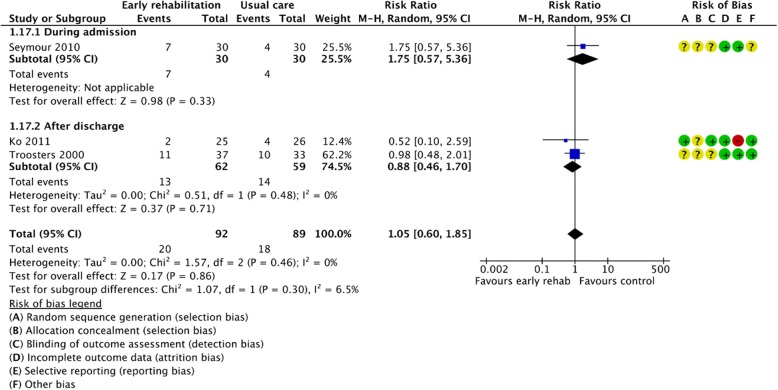
Results: We included 13 randomized trials (801 participants). Our meta-analyses showed a clinically relevant reduction in mortality after early PR (4 trials, 319 patients; RR = 0.58 (95% CI: [0.35 to 0.98])) and at the longest follow-up (3 trials, 127 patients; RR = 0.55 (95% CI: [0.12 to 2.57])). Early PR reduced number of days in hospital by 4.27 days (1 trial, 180 patients; 95% CI: [- 6.85 to - 1.69]) and hospital readmissions (6 trials, 319 patients; RR = 0.47 (95% CI: [0.29 to 0.75])). Moreover, early PR improved HRQoL and walking distance, and did not affect drop-out rate. Several of the trials had unclear risk of bias in regard to the randomization and blinding, for some outcome there was also a lack of power.
Conclusion: Moderate quality of evidence showed reductions in mortality, number of days in hospital and number of readmissions after early PR in patients hospitalized with a COPD exacerbation. Long-term effects on mortality were not statistically significant, but improvements in HRQoL and exercise capacity appeared to be maintained for at least 12 months. Therefore, we recommend early supervised PR to patients with COPD-related exacerbations. PR should be initiated during hospital admission or within 4 weeks after hospital discharge.
Keywords: Chronic obstructive pulmonary disease; Exacerbation of COPD; Hospital readmissions; Mortality; Supervised early pulmonary rehabilitation; Systematic review.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
