

The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990-2016
- PMID: 30219317
- PMCID: PMC6227386
- DOI: 10.1016/S2214-109X(18)30407-8
The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990-2016
Abstract
Background: The burden of cardiovascular diseases is increasing in India, but a systematic understanding of its distribution and time trends across all the states is not readily available. In this report, we present a detailed analysis of how the patterns of cardiovascular diseases and major risk factors have changed across the states of India between 1990 and 2016.
Methods: We analysed the prevalence and disability-adjusted life-years (DALYs) due to cardiovascular diseases and the major component causes in the states of India from 1990 to 2016, using all accessible data sources as part of the Global Burden of Diseases, Injuries, and Risk Factors Study 2016. We placed states into four groups based on epidemiological transition level (ETL), defined using the ratio of DALYs from communicable diseases to those from non-communicable diseases and injuries combined, with a low ratio denoting high ETL and vice versa. We assessed heterogeneity in the burden of major cardiovascular diseases across the states of India, and the contribution of risk factors to cardiovascular diseases. We calculated 95% uncertainty intervals (UIs) for the point estimates.
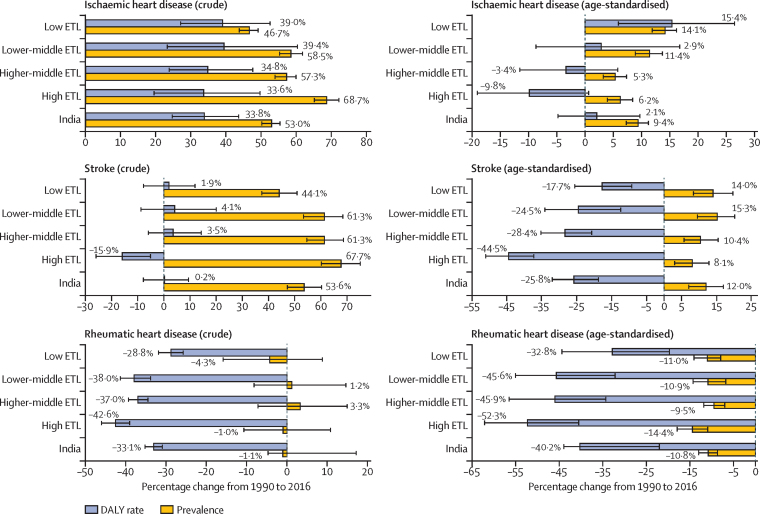
Findings: Overall, cardiovascular diseases contributed 28·1% (95% UI 26·5-29·1) of the total deaths and 14·1% (12·9-15·3) of the total DALYs in India in 2016, compared with 15·2% (13·7-16·2) and 6·9% (6·3-7·4), respectively, in 1990. In 2016, there was a nine times difference between states in the DALY rate for ischaemic heart disease, a six times difference for stroke, and a four times difference for rheumatic heart disease. 23·8 million (95% UI 22·6-25·0) prevalent cases of ischaemic heart disease were estimated in India in 2016, and 6·5 million (6·3-6·8) prevalent cases of stroke, a 2·3 times increase in both disorders from 1990. The age-standardised prevalence of both ischaemic heart disease and stroke increased in all ETL state groups between 1990 and 2016, whereas that of rheumatic heart disease decreased; the increase for ischaemic heart disease was highest in the low ETL state group. 53·4% (95% UI 52·6-54·6) of crude deaths due to cardiovascular diseases in India in 2016 were among people younger than 70 years, with a higher proportion in the low ETL state group. The leading overlapping risk factors for cardiovascular diseases in 2016 included dietary risks (56·4% [95% CI 48·5-63·9] of cardiovascular disease DALYs), high systolic blood pressure (54·6% [49·0-59·8]), air pollution (31·1% [29·0-33·4]), high total cholesterol (29·4% [24·3-34·8]), tobacco use (18·9% [16·6-21·3]), high fasting plasma glucose (16·7% [11·4-23·5]), and high body-mass index (14·7% [8·3-22·0]). The prevalence of high systolic blood pressure, high total cholesterol, and high fasting plasma glucose increased generally across all ETL state groups from 1990 to 2016, but this increase was variable across the states; the prevalence of smoking decreased during this period in all ETL state groups.
Interpretation: The burden from the leading cardiovascular diseases in India-ischaemic heart disease and stroke-varies widely between the states. Their increasing prevalence and that of several major risk factors in every part of India, especially the highest increase in the prevalence of ischaemic heart disease in the less developed low ETL states, indicates the need for urgent policy and health system response appropriate for the situation in each state.
Funding: Bill & Melinda Gates Foundation; and Indian Council of Medical Research, Department of Health Research, Ministry of Health and Family Welfare, Government of India.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures




Comment in
-
India's escalating burden of non-communicable diseases.Lancet Glob Health. 2018 Dec;6(12):e1262-e1263. doi: 10.1016/S2214-109X(18)30448-0. Epub 2018 Oct 3. Lancet Glob Health. 2018. PMID: 30292427 No abstract available.
References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. - PMC - PubMed
-
- Ralston J, Reddy KS, Fuster V, Narula J. Cardiovascular diseases on the global agenda: the United Nations high level meeting, Sustainable Development Goals, and the way forward. Glob Heart. 2016;11:375–379. - PubMed
-
- Joshi P, Islam S, Pais P. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA. 2007;297:286–294. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
