

Aicardi goutières syndrome is associated with pulmonary hypertension
- PMID: 30219631
- PMCID: PMC6880931
- DOI: 10.1016/j.ymgme.2018.09.004
Aicardi goutières syndrome is associated with pulmonary hypertension
Abstract
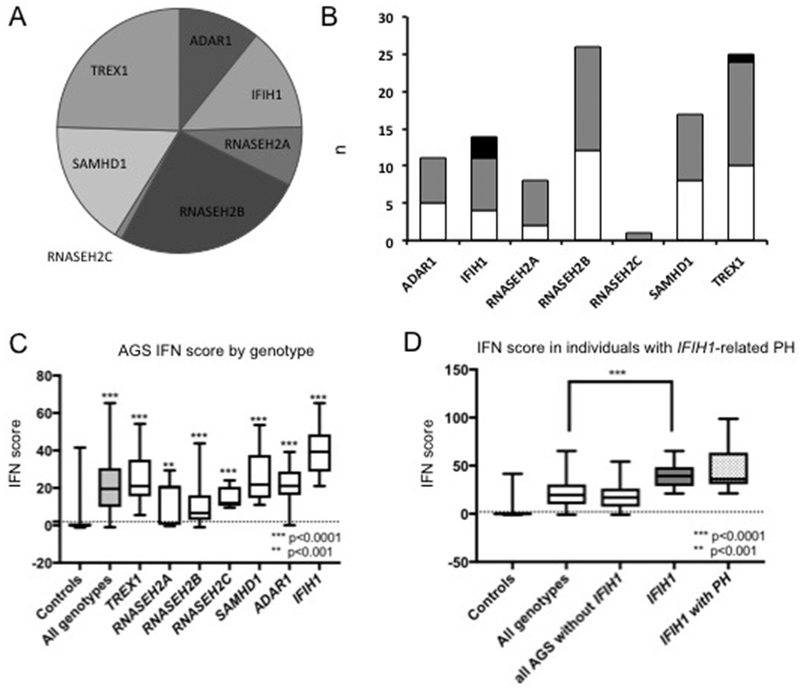
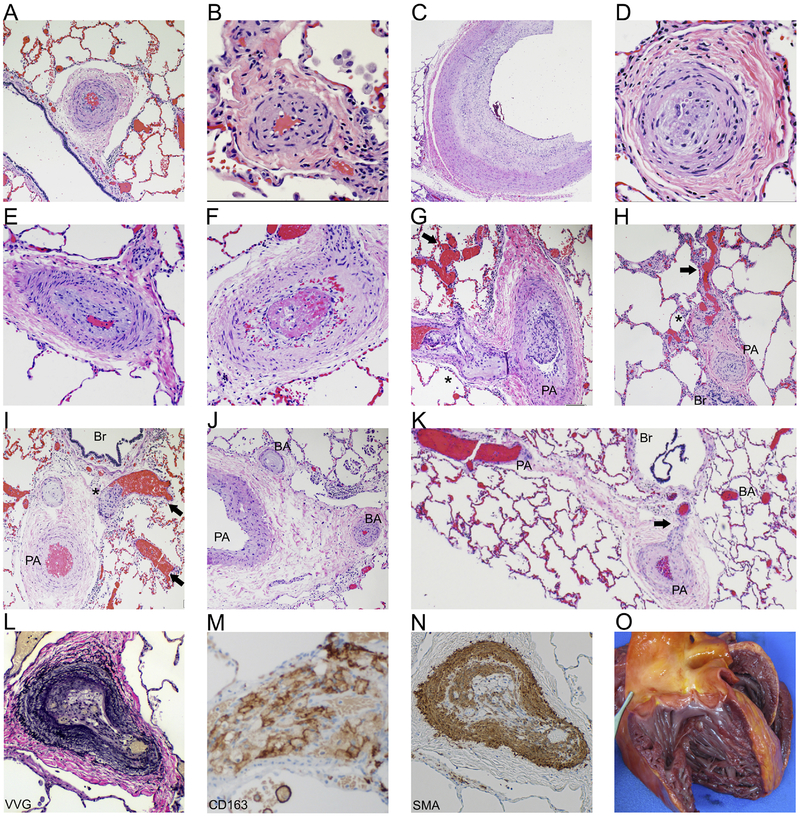
While pulmonary hypertension (PH) is a potentially life threatening complication of many inflammatory conditions, an association between Aicardi Goutières syndrome (AGS), a rare genetic cause of interferon (IFN) overproduction, and the development of PH has not been characterized to date. We analyzed the cardiac function of individuals with AGS enrolled in the Myelin Disorders Bioregistry Project using retrospective chart review (n = 61). Additional prospective echocardiograms were obtained when possible (n = 22). An IFN signature score, a marker of systemic inflammation, was calculated through the measurement of mRNA transcripts of type I IFN-inducible genes (interferon signaling genes or ISG). Pathologic analysis was performed as available from autopsy samples. Within our cohort, four individuals were identified to be affected by PH: three with pathogenic gain-of-function mutations in the IFIH1 gene and one with heterozygous TREX1 mutations. All studied individuals with AGS were noted to have elevated IFN signature scores (Mann-Whitney p < .001), with the highest levels in individuals with IFIH1 mutations (Mann-Whitney p < .0001). We present clinical and histologic evidence of PH in a series of four individuals with AGS, a rare interferonopathy. Importantly, IFIH1 and TREX1 may represent a novel cause of PH. Furthermore, these findings underscore the importance of screening all individuals with AGS for PH.
Keywords: Aicardi Goutières Syndrome; Interferons; Pulmonary hypertension.
Copyright © 2018. Published by Elsevier Inc.
Conflict of interest statement
Conflicts of Interest
LA, DBF, AG, AT, NU, ZC, CG, GH, UK, SK, DS, OS, BH: No conflicts to disclose
AV: receives support from Gilead Sciences Inc, Eli Lily and Company, Shire, and Ilumina Inc.
AC: consultant for Bracket Global, Inc and Ultragenyx Pharma, Inc.
Figures
References
-
- Huertas A, Perros F, Tu L, Cohen-Kaminsky S, Montani D, Dorfmuller P, et al. Immune dysregulation and endothelial dysfunction in pulmonary arterial hypertension: a complex interplay. Circulation. 2014;129(12):1332–40. - PubMed
-
- Bazan IS, Mensah KA, Rudkovskaia AA, Adonteng-Boateng PK, Herzog EL, Buckley L, et al. Pulmonary arterial hypertension in the setting of scleroderma is different than in the setting of lupus: A review. Respiratory medicine. 2018;134:42–6. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
