

Pharmacokinetic determinants of cisplatin-induced subclinical kidney injury in oncology patients
- PMID: 30220072
- PMCID: PMC6656531
- DOI: 10.1007/s00228-018-2552-z
Pharmacokinetic determinants of cisplatin-induced subclinical kidney injury in oncology patients
Abstract
Purpose: The ability to predict and detect clinical and subclinical nephrotoxicity early in the course of therapy has the potential to improve long-term outcomes in cancer patients receiving cisplatin chemotherapy. Pharmacokinetic parameters could serve as predictors of cisplatin-induced nephrotoxicity.
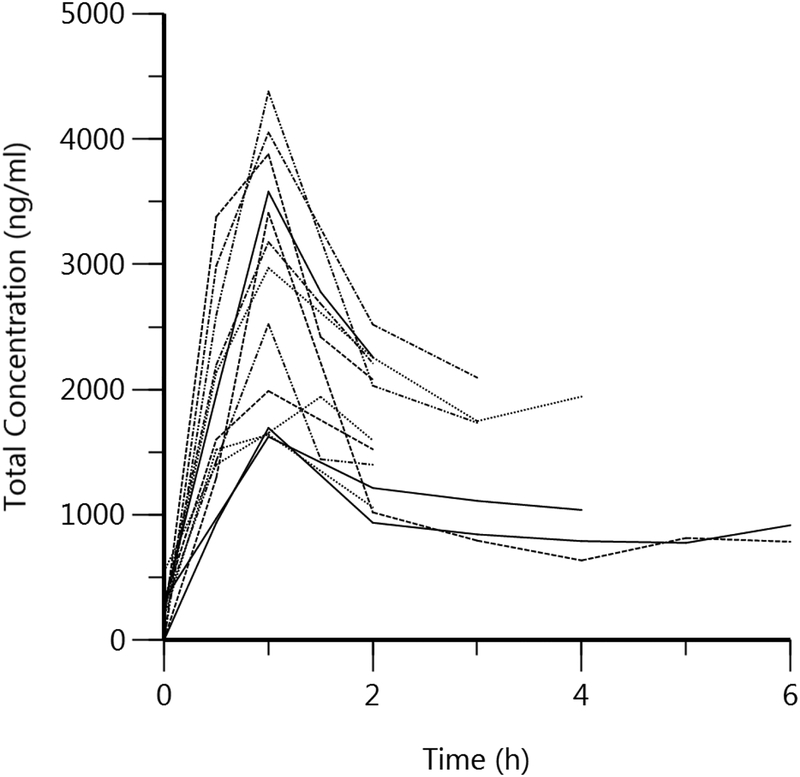
Methods: Participants [n = 13] were treated with a 1-h cisplatin infusion [30-75 mg/m2]. Blood was collected pre-dose and up to 6 h post-dose. Urinary biomarkers [KIM-1, calbindin, clusterin, GST-pi, β2M, albumin, NGAL, osteopontin, clusterin, MCP-1, cystatin C, and TFF3] were measured at baseline, days 3 and 10. Total and unbound platinum concentrations were measured using ICP/MS. Noncompartmental analysis was performed, and correlation and regression analyses evaluated the relationships between platinum pharmacokinetics and nephrotoxicity.
Results: Peak platinum urinary concentrations correlated with urinary levels of KIM-1, calbindin, clusterin, GST-pi, β2M, albumin, NGAL, osteopontin, clusterin, cystatin C, and TFF3 at day 10. Unbound platinum plasma concentrations at 2 h also correlated with urinary clusterin, β2M, cystatin C, NGAL, osteopontin, and TFF3 at day 3. Regression analyses suggested 2-h total plasma platinum concentrations greater than 2000 ng/ml, and peak urinary platinum concentrations above 24,000 ng/ml may serve as potential approximations for elevated risk of nephrotoxicity. Platinum area under the plasma concentration time curve was associated with serum creatinine and estimated glomerular filtration rate.
Conclusions: Peak plasma and urinary platinum concentrations and pharmacokinetic parameters were associated with risk of subclinical cisplatin-induced kidney injury as assessed using novel urinary biomarkers. Future studies will examine these relationships in larger clinical populations of cisplatin-induced acute kidney injury.
Keywords: Biomarkers; Cisplatin; Nephrotoxicity; Pharmacokinetics.
Conflict of interest statement
Conflict of Interest
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures

Similar articles
-
Pharmacokinetics of cisplatin and relation to nephrotoxicity in paediatric patients.Eur J Clin Pharmacol. 2001 Aug;57(5):393-402. doi: 10.1007/s002280100319. Eur J Clin Pharmacol. 2001. PMID: 11599657 Clinical Trial.
-
Understanding Cisplatin Pharmacokinetics and Toxicodynamics to Predict and Prevent Kidney Injury.J Pharmacol Exp Ther. 2024 Nov 19;391(3):399-414. doi: 10.1124/jpet.124.002287. J Pharmacol Exp Ther. 2024. PMID: 39322416 Review.
-
Urinary kidney injury molecule-1 and monocyte chemotactic protein-1 are noninvasive biomarkers of cisplatin-induced nephrotoxicity in lung cancer patients.Cancer Chemother Pharmacol. 2015 Nov;76(5):989-96. doi: 10.1007/s00280-015-2880-y. Epub 2015 Sep 25. Cancer Chemother Pharmacol. 2015. PMID: 26407820 Free PMC article. Clinical Trial.
-
Profiling of Kidney Injury Biomarkers in Patients Receiving Cisplatin: Time-dependent Changes in the Absence of Clinical Nephrotoxicity.Clin Pharmacol Ther. 2017 Apr;101(4):510-518. doi: 10.1002/cpt.606. Epub 2017 Feb 14. Clin Pharmacol Ther. 2017. PMID: 28002630 Free PMC article.
-
Time-dependent changes in kidney injury biomarkers in patients receiving multiple cycles of cisplatin chemotherapy.Toxicol Rep. 2020 Apr 22;7:571-576. doi: 10.1016/j.toxrep.2020.04.003. eCollection 2020. Toxicol Rep. 2020. PMID: 32382514 Free PMC article. Review.
Cited by
-
Early diagnostic biomarkers for acute kidney injury using cisplatin-induced nephrotoxicity in rat model.Curr Res Toxicol. 2023 Nov 7;5:100135. doi: 10.1016/j.crtox.2023.100135. eCollection 2023. Curr Res Toxicol. 2023. PMID: 38033659 Free PMC article.
-
Combined extracts of Curcuma longa and Curcuma zedoaria ameliorates cisplatin-induced kidney damage in rats.Open Vet J. 2025 Jan;15(1):428-436. doi: 10.5455/OVJ.2025.v15.i1.38. Epub 2025 Jan 31. Open Vet J. 2025. PMID: 40092179 Free PMC article.
-
Spatio-temporal transcriptomic analysis reveals distinct nephrotoxicity, DNA damage, and regeneration response after cisplatin.Cell Biol Toxicol. 2025 Feb 21;41(1):49. doi: 10.1007/s10565-025-10003-z. Cell Biol Toxicol. 2025. PMID: 39982567 Free PMC article.
-
Natural products: potential treatments for cisplatin-induced nephrotoxicity.Acta Pharmacol Sin. 2021 Dec;42(12):1951-1969. doi: 10.1038/s41401-021-00620-9. Epub 2021 Mar 9. Acta Pharmacol Sin. 2021. PMID: 33750909 Free PMC article. Review.
-
Optimized Dosing: The Next Step in Precision Medicine in Non-Small-Cell Lung Cancer.Drugs. 2022 Jan;82(1):15-32. doi: 10.1007/s40265-021-01654-3. Epub 2021 Dec 11. Drugs. 2022. PMID: 34894338 Review.
References
-
- Pabla N and Dong Z, Cisplatin nephrotoxicity: mechanisms and renoprotective strategies. Kidney Int, 2008. 73(9): p. 994–1007. - PubMed
-
- Arany I and Safirstein RL, Cisplatin nephrotoxicity. Semin Nephrol, 2003. 23(5): p. 460–4. - PubMed
-
- Khwaja A, KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract, 2012. 120(4): p. c179–84. - PubMed
-
- Dieterle F, et al., Renal biomarker qualification submission: a dialog between the FDA-EMEA and Predictive Safety Testing Consortium. Nat Biotechnol, 2010. 28(5): p. 455–62. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
