

Primary and Secondary Diastolic Dysfunction in Heart Failure With Preserved Ejection Fraction
- PMID: 30220416
- PMCID: PMC6608585
- DOI: 10.1016/j.amjcard.2018.07.012
Primary and Secondary Diastolic Dysfunction in Heart Failure With Preserved Ejection Fraction
Abstract
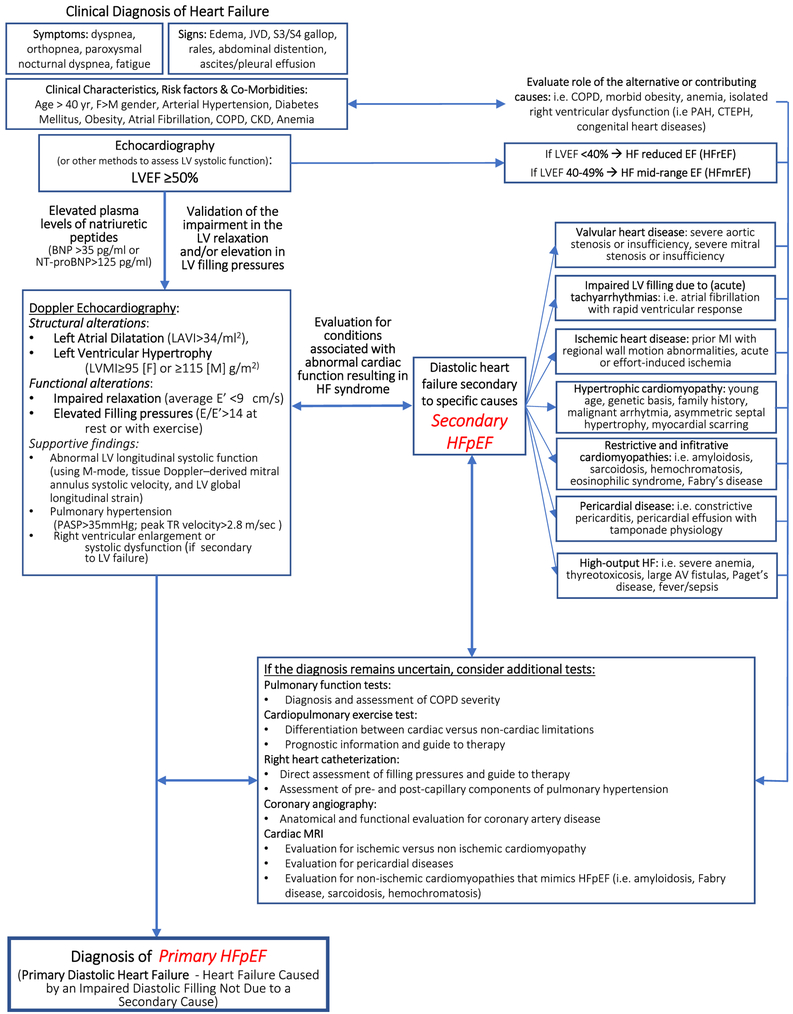
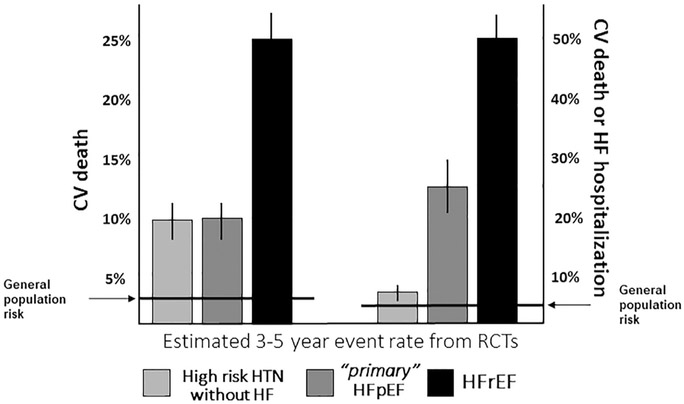
Approximately 50% of patients with symptoms and signs of heart failure have a left ventricular ejection fraction (LVEF) ≥50% and are often simply referred to as 'heart failure with preserved EF', 'HFpEF'. Many of such patients have HF secondary to specific cardiac conditions (i.e., valvular or pericardial disease) in which the symptoms and signs occur despite the LVEF being preserved due to diastolic dysfunction secondary to the underlying disease (secondary HFpEF), differently from those HFpEF patients in which the impaired LV filling is due to a primary diastolic dysfunction (primary HFpEF). When primary HFpEF patients are properly diagnosed, they appear to have a milder form of HF with a lower cardiovascular mortality compared with HFrEF and secondary HFpEF population, but a risk of HF hospitalization that is significantly higher than patients with similar cardiovascular risk factors but without the diagnosis of HFpEF. We herein review the diagnostic approach to HFpEF and present a differential diagnosis of HFpEF in a primary and secondary form.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures
The authors have no conflicts of interest to disclose.
Figures


Similar articles
-
Comparison of Prognostic Usefulness of Serum Insulin-Like Growth Factor-Binding Protein 7 in Patients With Heart Failure and Preserved Versus Reduced Left Ventricular Ejection Fraction.Am J Cardiol. 2018 Jun 15;121(12):1558-1566. doi: 10.1016/j.amjcard.2018.02.041. Epub 2018 Mar 14. Am J Cardiol. 2018. PMID: 29622288
-
Biomarker Profiles in Heart Failure Patients With Preserved and Reduced Ejection Fraction.J Am Heart Assoc. 2017 Mar 30;6(4):e003989. doi: 10.1161/JAHA.116.003989. J Am Heart Assoc. 2017. PMID: 28360225 Free PMC article.
-
Update on diastolic heart failure or heart failure with preserved ejection fraction in the older adults.Ann Med. 2013 Feb;45(1):37-50. doi: 10.3109/07853890.2012.660493. Epub 2012 Mar 13. Ann Med. 2013. PMID: 22413912 Review.
-
How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC).Eur Heart J. 2019 Oct 21;40(40):3297-3317. doi: 10.1093/eurheartj/ehz641. Eur Heart J. 2019. PMID: 31504452
-
Valvular Disease and Heart Failure with Preserved Ejection Fraction.Heart Fail Clin. 2021 Jul;17(3):387-395. doi: 10.1016/j.hfc.2021.02.005. Heart Fail Clin. 2021. PMID: 34051971 Review.
Cited by
-
An overview of radiation-induced heart disease.Radiat Oncol J. 2022 Jun;40(2):89-102. doi: 10.3857/roj.2021.00766. Epub 2022 Jun 21. Radiat Oncol J. 2022. PMID: 35796112 Free PMC article.
-
Ischemic Cardiomyopathy and Heart Failure After Acute Myocardial Infarction.Curr Cardiol Rep. 2022 Oct;24(10):1505-1515. doi: 10.1007/s11886-022-01766-6. Epub 2022 Aug 16. Curr Cardiol Rep. 2022. PMID: 35972638 Free PMC article. Review.
-
Abnormal left ventricular subendocardial perfusion and diastolic function in women with obesity and heart failure and preserved ejection fraction.Int J Cardiovasc Imaging. 2023 Apr;39(4):811-819. doi: 10.1007/s10554-022-02782-x. Epub 2023 Jan 6. Int J Cardiovasc Imaging. 2023. PMID: 36607469 Free PMC article.
-
A State of Natriuretic Peptide Deficiency.Endocr Rev. 2023 May 8;44(3):379-392. doi: 10.1210/endrev/bnac029. Endocr Rev. 2023. PMID: 36346821 Free PMC article.
-
Symptom Perception and Influencing Factors in Chinese Patients with Heart Failure: A Preliminary Exploration.Int J Environ Res Public Health. 2020 Apr 14;17(8):2692. doi: 10.3390/ijerph17082692. Int J Environ Res Public Health. 2020. PMID: 32295183 Free PMC article.
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL. American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of HF: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013;128:e240–327. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. Authors/Task Force Members; Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016;18:891–975. - PubMed
-
- Nagueh SF, Smiseth OA, Appleton CP, ByrdBF Dokainish H 3rd, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Popescu BA, Waggoner AD. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2016;29:277–314. 10.1016/j.echo.2016.01.011. - DOI - PubMed
-
- Kalogeropoulos AP, Fonarow GC, Georgiopoulou V, Burkman G, Siwamogsatham S, Patel A, Li S, Papadimitriou L, Butler J. Characteristics and outcomes of adult outpatients with heart failure and improved or recovered ejection fraction. JAMA Cardiol 2016;1:510–518. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
