

Temporality of heparin-induced antibodies: a retrospective study in outpatients undergoing hemodialysis on unfractionated heparin
- PMID: 30221035
- PMCID: PMC6137914
- DOI: 10.1186/s40164-018-0115-8
Temporality of heparin-induced antibodies: a retrospective study in outpatients undergoing hemodialysis on unfractionated heparin
Abstract
Background: Heparin-induced antibodies (HIA) are responsible for causing heparin-induced thrombocytopenia and thrombosis. Research has shown that the temporality of heparin-induced antibodies does not follow the classic immunologic response. The immunobiology of HIA generation remains unclear with varying in vitro and in vivo data. Outpatients undergoing hemodialysis (HD) are exposed to heparin chronically. The HIA immune response can therefore be investigated in vivo in this population.
Methods: We examined the time between the start of HD using unfractionated heparin and HIA levels in 212 outpatients during a 6-year period. Antibodies were detected on enzyme-linked immunosorbent assay. HIA levels were analyzed to determine significance of the trend over time. HIA subgroups were also analyzed for correlation with subsequent thrombotic events and platelet count during follow up.
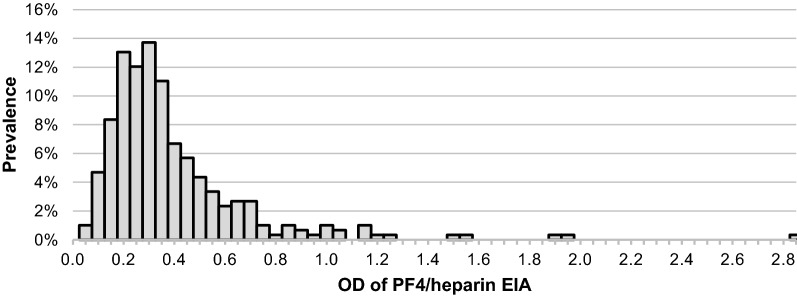
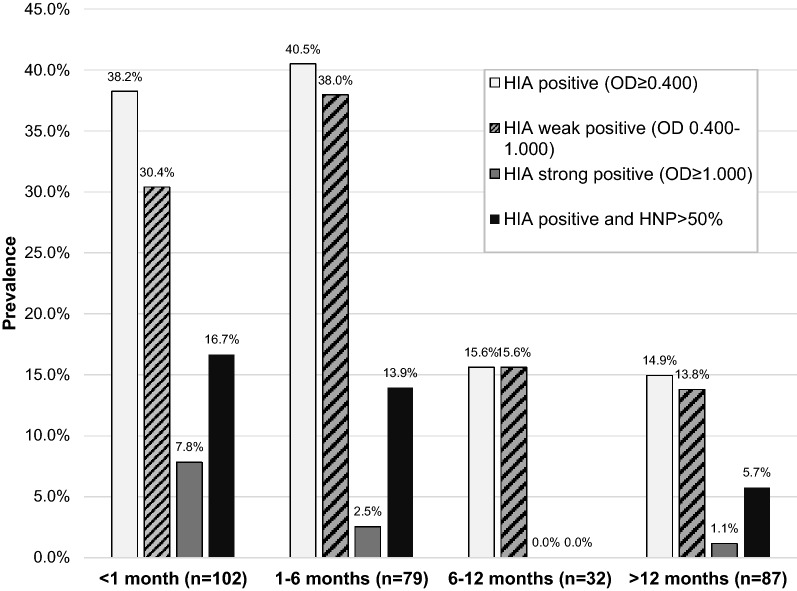
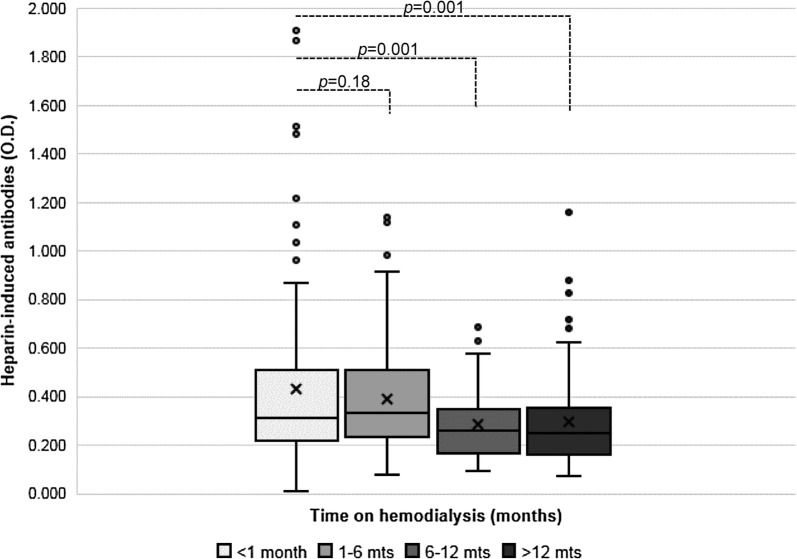
Results: Overall, the HIA response in HD was found to peak early with waning antibody response despite continued exposure to heparin. The peak prevalence of a strong immune response (optical density > 1.000) was early and short lived, while weaker immune response (optical density 0.400-1.000) persisted for the first 6 months then declined. The mean follow-up time per patient was 2.3 ± 1.4 years. Despite circulating HIA, including high titers, no patients developed HIT in this sample. There was no association between HIA and thrombocytopenia. There was increased incidence of thrombosis in patients with strong HIA compared to other groups, but this did not achieve statistical significance.
Conclusions: The data suggest a significant temporal pattern of HIA in outpatients undergoing HD using unfractionated heparin. Positive HIA was not found to be significantly associated with thrombocytopenia or thrombosis risk in these patients. However, while not achieving statistical significance, subsequent thrombotic events occurred most frequently in the strong positive HIA group (optical density > 1.000). Further research into HIA and risk of thrombosis in this population is needed.
Keywords: Antibodies; HIT; Hemodialysis; Heparin; Thrombocytopenia; Thrombosis.
Figures
Similar articles
-
Prevalence of heparin-induced antibodies in patients with chronic renal failure undergoing hemodialysis.J Clin Lab Anal. 2005;19(5):189-95. doi: 10.1002/jcla.20076. J Clin Lab Anal. 2005. PMID: 16170812 Free PMC article.
-
Prevalence and clinical significance of heparin induced antibodies in chronic hemodialysis patients and cardiac surgery patients.Int J Artif Organs. 2011 Dec;34(12):1172-8. doi: 10.5301/ijao.5000020. Int J Artif Organs. 2011. PMID: 22198603
-
Prevalence of heparin-induced antibody in African-American hemodialysis patients--comparison to non-dialysis patients.Clin Nephrol. 2009 Mar;71(3):263-6. doi: 10.5414/cnp71263. Clin Nephrol. 2009. PMID: 19281736
-
Recognition and management of heparin-induced thrombocytopenia (HIT) and thrombosis.Semin Thromb Hemost. 1997;23(6):569-74. doi: 10.1055/s-2007-996138. Semin Thromb Hemost. 1997. PMID: 9469632 Review.
-
Spontaneous HIT syndrome post-knee replacement surgery with delayed recovery of thrombocytopenia: a case report and literature review.Platelets. 2017 Sep;28(6):614-620. doi: 10.1080/09537104.2017.1366973. Epub 2017 Aug 31. Platelets. 2017. PMID: 28856946 Review.
Cited by
-
Heparin-induced thrombocytopenia in end-stage renal disease: Reliability of the PF4-heparin ELISA.Res Pract Thromb Haemost. 2021 Aug 4;5(5):e12573. doi: 10.1002/rth2.12573. eCollection 2021 Jul. Res Pract Thromb Haemost. 2021. PMID: 34386689 Free PMC article.
-
Heparin-Induced Thrombocytopenia in Chronic Hemodialysis Patients.Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296231177993. doi: 10.1177/10760296231177993. Clin Appl Thromb Hemost. 2023. PMID: 37253454 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
