

Development of a dedicated phantom for multi-target single-isocentre stereotactic radiosurgery end to end testing
- PMID: 30221462
- PMCID: PMC6236824
- DOI: 10.1002/acm2.12452
Development of a dedicated phantom for multi-target single-isocentre stereotactic radiosurgery end to end testing
Abstract
Purpose: The aim of this project was to design and manufacture a cost-effective end-to-end (E2E) phantom for quantifying the geometric and dosimetric accuracy of a linear accelerator based, multi-target single-isocenter (MTSI) frameless stereotactic radiosurgery (SRS) technique.
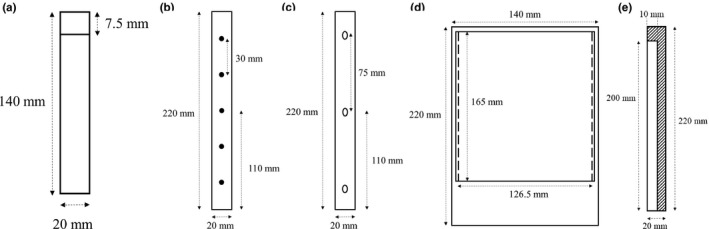
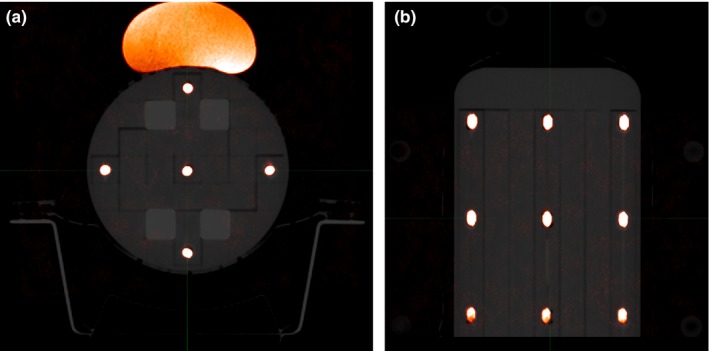
Method: A perspex Multi-Plug device from a Sun Nuclear ArcCheck phantom (Sun Nuclear, Melbourne, FL) was enhanced to make it more applicable for MTSI SRS E2E testing. The following steps in the SRS chain were then analysed using the phantom: magnetic resonance imaging (MRI) distortion, planning computed tomography (CT) scan and MRI image registration accuracy, phantom setup accuracy using CBCT, dosimetric accuracy using ion chamber, planar film dose measurements and coincidence of linear accelerator mega-voltage (MV), and kilo-voltage (kV) isocenters using Winston-Lutz testing (WLT).
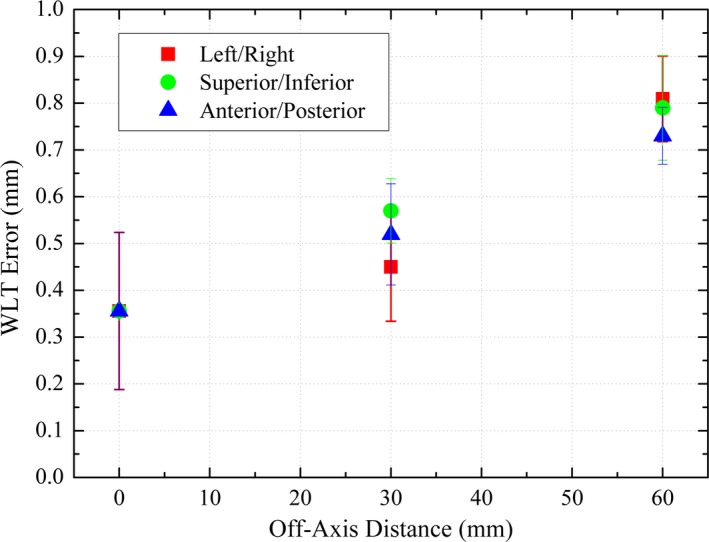
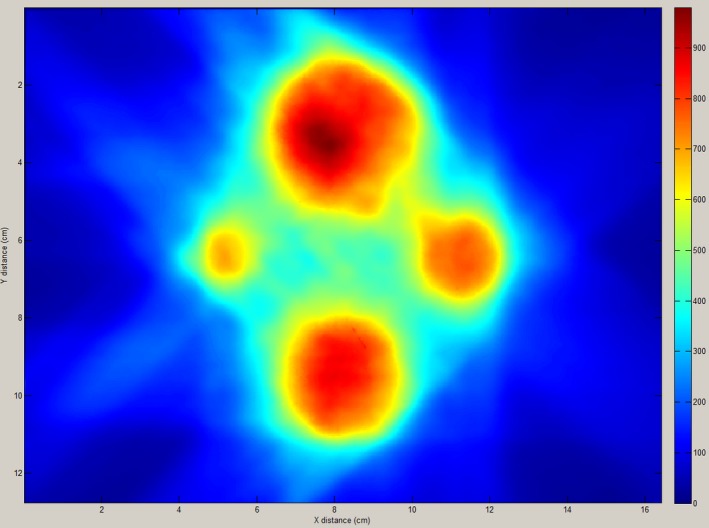
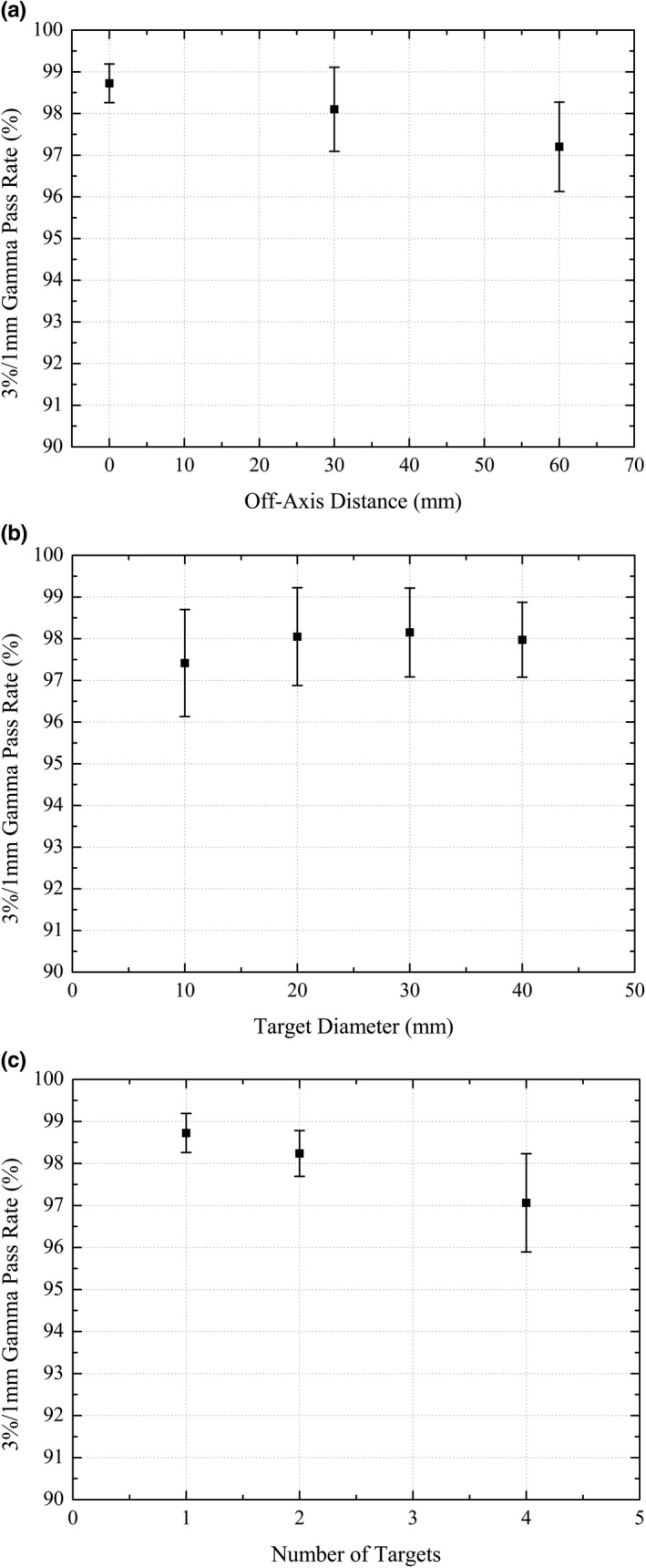
Results: The dedicated E2E phantom was able to successfully quantify the geometric and dosimetric accuracy of the MTSI SRS technique. MRI distortions were less than 0.5 mm, or half a voxel size. The average MRI-CT registration accuracy was 0.15 mm (±0.31 mm), 0.20 mm (±0.16 mm), and 0.39 mm (±0.11 mm) in the superior/inferior, left/right and, anterior/posterior directions, respectively. The phantom setup accuracy using CBCT was better than 0.2 mm and 0.1°. Point dose measurements were within 5% of the treatment planning system predicted dose. The comparison of planar film doses to the planning system dose distributions, performed using gamma analysis, resulted in pass rates greater than 97% for 3%/1 mm gamma criteria. Finally, off-axis WLT showed MV/kV coincidence to be within 1 mm for off-axis distances up to 60 mm.
Conclusion: A novel, versatile and cost-effective phantom for comprehensive E2E testing of MTSI SRS treatments was developed, incorporating multiple detector types and fiducial markers. The phantom is capable of quantifying the accuracy of each step in the MTSI SRS planning and treatment process.
Keywords: MRI deformation; dosimetric validation; end-to-end testing; multi-target; single isocentre; stereotactic radiosurgery.
© 2018 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Figures



References
-
- Chin LS, Regine WF. Principles and Practice of Stereotactic Radiosurgery. Berlin: Springer Science & Business Media; 2010.
-
- Lohr F, Pirzkall A, Hof H, Fleckenstein K, Debus J. Adjuvant treatment of brain metastases. Paper presented at: Seminars in surgical oncology; 2001. - PubMed
-
- Clark GM, Popple RA, Prendergast BM, et al. Plan quality and treatment planning technique for single isocenter cranial radiosurgery with volumetric modulated arc therapy. Pract Radiat Oncol. 2012;2:306–313. - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole‐brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006;295:2483–2491. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
