

Biopsy-Proven Small-Fiber Neuropathy in Primary Sjögren's Syndrome: Neuropathic Pain Characteristics, Autoantibody Findings, and Histopathologic Features
- PMID: 30221483
- PMCID: PMC7556316
- DOI: 10.1002/acr.23762
Biopsy-Proven Small-Fiber Neuropathy in Primary Sjögren's Syndrome: Neuropathic Pain Characteristics, Autoantibody Findings, and Histopathologic Features
Erratum in
-
Erratum.Arthritis Care Res (Hoboken). 2019 Sep;71(9):1283. doi: 10.1002/acr.24041. Arthritis Care Res (Hoboken). 2019. PMID: 31469257 No abstract available.
Abstract
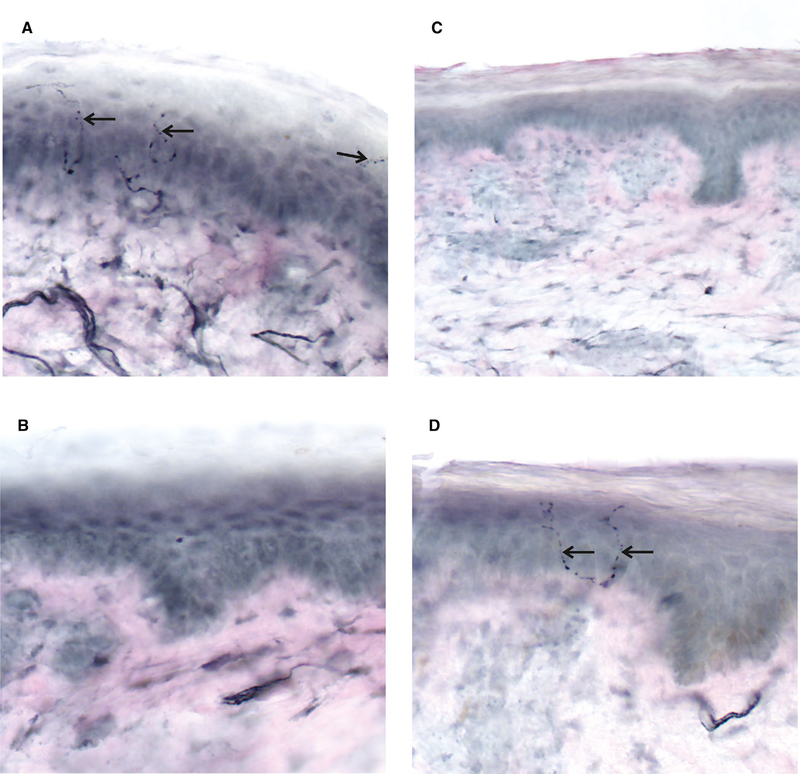
Objective: Painful small-fiber neuropathies (SFNs) in primary Sjögren's syndrome (SS) may present as pure or mixed with concurrent large-fiber involvement. SFN can be diagnosed by punch skin biopsy results that identify decreased intra-epidermal nerve-fiber density (IENFD) of unmyelinated nerves.
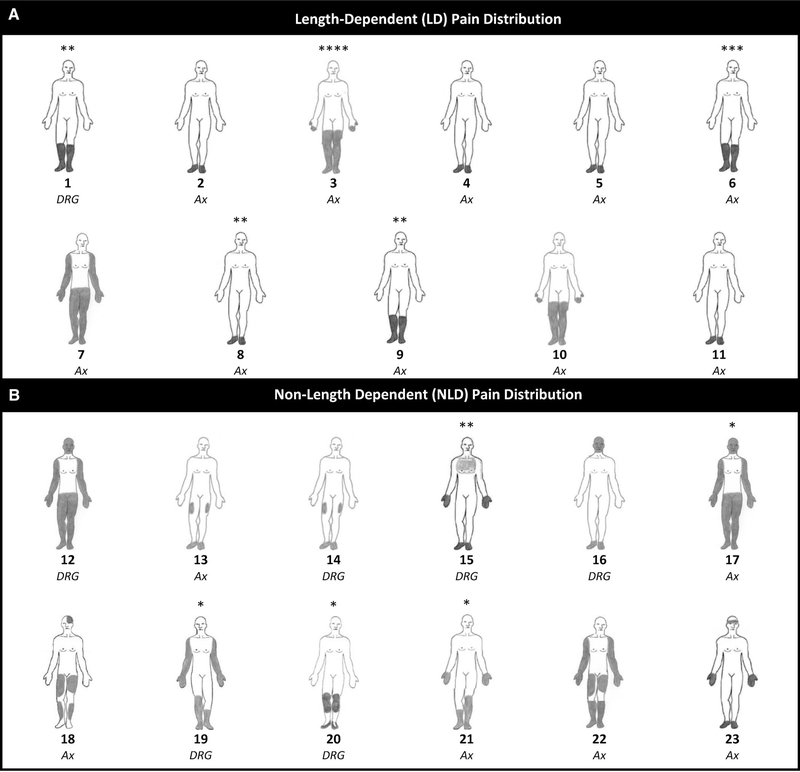
Methods: We compared 23 consecutively evaluated patients with SS with pure and mixed SFN versus 98 patients without SFN. We distinguished between markers of dorsal root ganglia (DRG) degeneration (decreased IENFD in the proximal thigh versus the distal leg) versus axonal degeneration (decreased IENFD in the distal leg versus the proximal thigh).
Results: There were no differences in pain intensity, pain quality, and treatment characteristics in the comparison of 13 patients with pure SFN versus 10 patients with mixed SFN. Ten patients with SFN (approximately 45%) had neuropathic pain preceding sicca symptoms. Opioid analgesics were prescribed to approximately 45% of patients with SFN. When compared to 98 patients without SFN, the 23 patients with SFN had an increased frequency of male sex (30% versus 9%; P < 0.01), a decreased frequency of anti-Ro 52 (P = 0.01) and anti-Ro 60 antibodies (P = 0.01), rheumatoid factor positivity (P < 0.01), and polyclonal gammopathy (P < 0.01). Eleven patients had stocking-and-glove pain, and 12 patients had nonstocking-and-glove pain. Skin biopsy results disclosed patterns of axonal (16 patients) and DRG injury (7 patients).
Conclusion: SS SFN had an increased frequency among male patients, a decreased frequency of multiple antibodies, frequent treatment with opioid analgesics, and the presence of nonstocking-and-glove pain. Distinguishing between DRG versus axonal injury is significant, especially given that mechanisms targeting the DRG may result in irreversible neuronal cell death. Altogether, these findings highlight clinical, autoantibody, and pathologic features that can help to define mechanisms and treatment strategies.
© 2018, American College of Rheumatology.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
Use of a novel high-resolution magnetic resonance neurography protocol to detect abnormal dorsal root Ganglia in Sjögren patients with neuropathic pain: case series of 10 patients and review of the literature.Medicine (Baltimore). 2014 May;93(3):121-134. doi: 10.1097/MD.0000000000000024. Medicine (Baltimore). 2014. PMID: 24797167 Free PMC article.
-
Characterization of Neuropathic Pain in Primary Sjögren's Syndrome with Respect to Neurophysiological Evidence of Small-Fiber Neuropathy.Pain Med. 2019 May 1;20(5):979-987. doi: 10.1093/pm/pny183. Pain Med. 2019. PMID: 30247738
-
The Clinical Features of Painful Small-Fiber Neuropathy Suggesting an Origin Linked to Primary Sjögren's Syndrome.Pain Pract. 2019 Apr;19(4):426-434. doi: 10.1111/papr.12763. Epub 2019 Feb 6. Pain Pract. 2019. PMID: 30636091
-
[Sjogren's syndrome-associated neuropathy].Brain Nerve. 2013 Nov;65(11):1333-42. Brain Nerve. 2013. PMID: 24200611 Review. Japanese.
-
Non-length-dependent small fiber neuropathy: Not a matter of stockings and gloves.Muscle Nerve. 2022 Jan;65(1):10-28. doi: 10.1002/mus.27379. Epub 2021 Aug 9. Muscle Nerve. 2022. PMID: 34374103 Review.
Cited by
-
Exploring the mechanisms of action of Zengye decoction (ZYD) against Sjogren's syndrome (SS) using network pharmacology and animal experiment.Pharm Biol. 2023 Dec;61(1):1286-1297. doi: 10.1080/13880209.2023.2248188. Pharm Biol. 2023. PMID: 37606264 Free PMC article.
-
Update on Sjögren's Syndrome 2018.Mediterr J Rheumatol. 2018 Dec 18;29(4):193-198. doi: 10.31138/mjr.29.4.193. eCollection 2018 Dec. Mediterr J Rheumatol. 2018. PMID: 32185326 Free PMC article. Review.
-
Peripheral Neuropathy in Systemic Autoimmune Rheumatic Diseases-Diagnosis and Treatment.Pharmaceuticals (Basel). 2023 Apr 14;16(4):587. doi: 10.3390/ph16040587. Pharmaceuticals (Basel). 2023. PMID: 37111344 Free PMC article. Review.
-
Sjögren's syndrome with and without neurological involvement.J Neurol. 2023 Jun;270(6):2987-2996. doi: 10.1007/s00415-023-11613-5. Epub 2023 Feb 18. J Neurol. 2023. PMID: 36802030 Free PMC article.
-
Sjogren Syndrome-Associated Autonomic Neuropathy.Cureus. 2022 Jun 1;14(6):e25563. doi: 10.7759/cureus.25563. eCollection 2022 Jun. Cureus. 2022. PMID: 35784971 Free PMC article.
References
-
- Birnbaum J. Peripheral nervous system manifestations of Sjogren syndrome: clinical patterns, diagnostic paradigms, etiopathogenesis, and therapeutic strategies. Neurologist 2010;16:287–97. - PubMed
-
- Pavlakis PP, Alexopoulos H, Kosmidis ML, Stamboulis E, Routsias JG, Tzartos SJ, et al. Peripheral neuropathies in Sjogren syndrome: a new reappraisal. J Neurol Neurosurg Psychiatry 2011;82:798–802. - PubMed
-
- Chan AC, Wilder-Smith EP. Small fiber neuropathy: getting bigger! Muscle Nerve 2016;53:671–82. - PubMed
-
- Chai J, Herrmann DN, Stanton M, Barbano RL, Logigian EL. Painful small-fiber neuropathy in Sjogren syndrome. Neurology 2005;65:925–7. - PubMed
-
- Ebenezer GJ, Hauer P, Gibbons C, McArthur JC, Polydefkis M. Assessment of epidermal nerve fibers: a new diagnostic and predictive tool for peripheral neuropathies. J Neuropathol Exp Neurol 2007;66:1059–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
