

Effect of Aspirin on All-Cause Mortality in the Healthy Elderly
- PMID: 30221595
- PMCID: PMC6433466
- DOI: 10.1056/NEJMoa1803955
Effect of Aspirin on All-Cause Mortality in the Healthy Elderly
Abstract
Background: In the primary analysis of the Aspirin in Reducing Events in the Elderly (ASPREE) trial, now published in the Journal, we report that the daily use of aspirin did not provide a benefit with regard to the primary end point of disability-free survival among older adults. A numerically higher rate of the secondary end point of death from any cause was observed with aspirin than with placebo.
Methods: From 2010 through 2014, we enrolled community-dwelling persons in Australia and the United States who were 70 years of age or older (or ≥65 years of age among blacks and Hispanics in the United States) and did not have cardiovascular disease, dementia, or disability. Participants were randomly assigned to receive 100 mg of enteric-coated aspirin or placebo. Deaths were classified according to the underlying cause by adjudicators who were unaware of trial-group assignments. Hazard ratios were calculated to compare mortality between the aspirin group and the placebo group, and post hoc exploratory analyses of specific causes of death were performed.
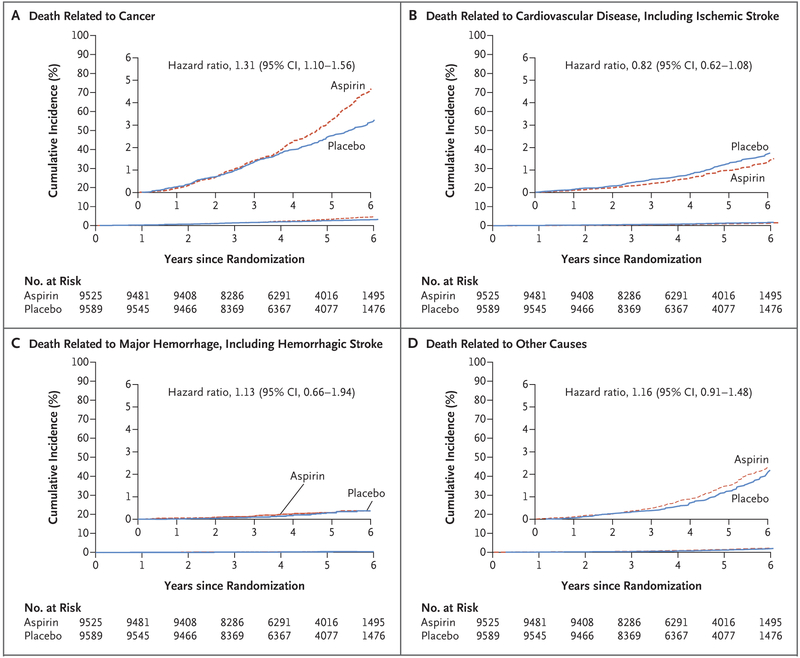
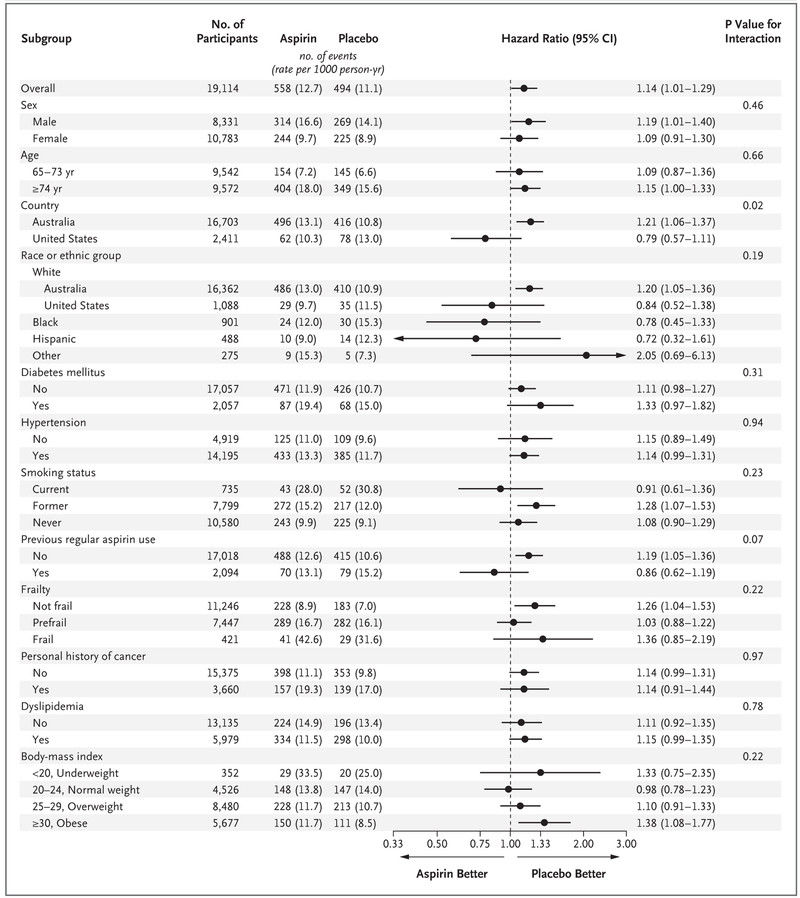
Results: Of the 19,114 persons who were enrolled, 9525 were assigned to receive aspirin and 9589 to receive placebo. A total of 1052 deaths occurred during a median of 4.7 years of follow-up. The risk of death from any cause was 12.7 events per 1000 person-years in the aspirin group and 11.1 events per 1000 person-years in the placebo group (hazard ratio, 1.14; 95% confidence interval [CI], 1.01 to 1.29). Cancer was the major contributor to the higher mortality in the aspirin group, accounting for 1.6 excess deaths per 1000 person-years. Cancer-related death occurred in 3.1% of the participants in the aspirin group and in 2.3% of those in the placebo group (hazard ratio, 1.31; 95% CI, 1.10 to 1.56).
Conclusions: Higher all-cause mortality was observed among apparently healthy older adults who received daily aspirin than among those who received placebo and was attributed primarily to cancer-related death. In the context of previous studies, this result was unexpected and should be interpreted with caution. (Funded by the National Institute on Aging and others; ASPREE ClinicalTrials.gov number, NCT01038583 .).
Figures
Comment in
-
Aspirin and Cancer Prevention in the Elderly: Where Do We Go From Here?Gastroenterology. 2019 Feb;156(3):534-538. doi: 10.1053/j.gastro.2018.11.063. Epub 2018 Dec 4. Gastroenterology. 2019. PMID: 30529298 No abstract available.
-
[Importance of acetylsalicylic acid in primary prevention : ASCEND, ARRIVE and ASPREE as well as a meta-analysis by Rothwell et al.].Internist (Berl). 2019 Feb;60(2):209-216. doi: 10.1007/s00108-018-0541-z. Internist (Berl). 2019. PMID: 30645666 German. No abstract available.
-
Requiem für ASS in der Primärprävention.MMW Fortschr Med. 2019 Feb;161(2):35. doi: 10.1007/s15006-019-0127-2. MMW Fortschr Med. 2019. PMID: 30721495 Review. German. No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042833 No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042834 No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775-1776. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042835 No abstract available.
References
-
- Ikeda Y, Shimada K, Teramoto T, et al. Low-dose aspirin for primary prevention of cardiovascular events in Japanese patients 60 years or older with atherosclerotic risk factors: a randomized clinical trial. JAMA 2014;312:2510–20. - PubMed
-
- Fowkes FGR, Price JF, Stewart MCW, et al. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: a randomized controlled trial. JAMA 2010;303:841–8. - PubMed
-
- Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA 2008;300:2134–41. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical