

Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly
- PMID: 30221597
- PMCID: PMC6289056
- DOI: 10.1056/NEJMoa1805819
Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly
Abstract
Background: Aspirin is a well-established therapy for the secondary prevention of cardiovascular events. However, its role in the primary prevention of cardiovascular disease is unclear, especially in older persons, who have an increased risk.
Methods: From 2010 through 2014, we enrolled community-dwelling men and women in Australia and the United States who were 70 years of age or older (or ≥65 years of age among blacks and Hispanics in the United States) and did not have cardiovascular disease, dementia, or disability. Participants were randomly assigned to receive 100 mg of enteric-coated aspirin or placebo. The primary end point was a composite of death, dementia, or persistent physical disability; results for this end point are reported in another article in the Journal. Secondary end points included major hemorrhage and cardiovascular disease (defined as fatal coronary heart disease, nonfatal myocardial infarction, fatal or nonfatal stroke, or hospitalization for heart failure).
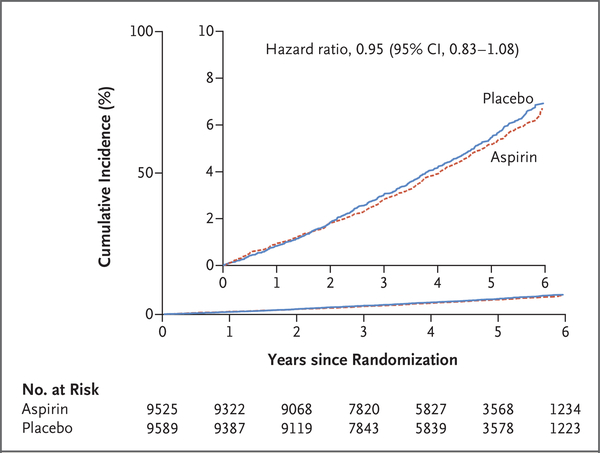
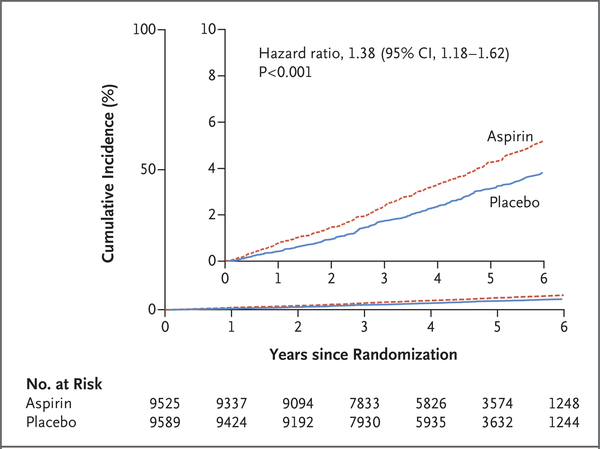
Results: Of the 19,114 persons who were enrolled in the trial, 9525 were assigned to receive aspirin and 9589 to receive placebo. After a median of 4.7 years of follow-up, the rate of cardiovascular disease was 10.7 events per 1000 person-years in the aspirin group and 11.3 events per 1000 person-years in the placebo group (hazard ratio, 0.95; 95% confidence interval [CI], 0.83 to 1.08). The rate of major hemorrhage was 8.6 events per 1000 person-years and 6.2 events per 1000 person-years, respectively (hazard ratio, 1.38; 95% CI, 1.18 to 1.62; P<0.001).
Conclusions: The use of low-dose aspirin as a primary prevention strategy in older adults resulted in a significantly higher risk of major hemorrhage and did not result in a significantly lower risk of cardiovascular disease than placebo. (Funded by the National Institute on Aging and others; ASPREE ClinicalTrials.gov number, NCT01038583 .).
Figures
Comment in
-
Aspirin and Cancer Prevention in the Elderly: Where Do We Go From Here?Gastroenterology. 2019 Feb;156(3):534-538. doi: 10.1053/j.gastro.2018.11.063. Epub 2018 Dec 4. Gastroenterology. 2019. PMID: 30529298 No abstract available.
-
[Importance of acetylsalicylic acid in primary prevention : ASCEND, ARRIVE and ASPREE as well as a meta-analysis by Rothwell et al.].Internist (Berl). 2019 Feb;60(2):209-216. doi: 10.1007/s00108-018-0541-z. Internist (Berl). 2019. PMID: 30645666 German. No abstract available.
-
Requiem für ASS in der Primärprävention.MMW Fortschr Med. 2019 Feb;161(2):35. doi: 10.1007/s15006-019-0127-2. MMW Fortschr Med. 2019. PMID: 30721495 Review. German. No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042833 No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042834 No abstract available.
-
Effects of Aspirin in the Healthy Elderly.N Engl J Med. 2019 May 2;380(18):1775-1776. doi: 10.1056/NEJMc1901774. N Engl J Med. 2019. PMID: 31042835 No abstract available.
-
Should aspirin be used for primary prevention in the healthy elderly?Evid Based Nurs. 2019 Oct;22(4):115. doi: 10.1136/ebnurs-2018-103041. Epub 2019 Jun 1. Evid Based Nurs. 2019. PMID: 31154354 No abstract available.
-
PURL: Aspirin, Yes, for at-risk elderly-but what about the healthy elderly?J Fam Pract. 2020 Apr;69(3):E16-E18. J Fam Pract. 2020. PMID: 32289133 Free PMC article.
References
-
- Australian Bureau of Statistics. 3303.0 — causes of death, Australia, 2016. (www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/3303.02016?OpenDocument).
-
- Centers for Disease Control and Prevention. LCWK3 — deaths, percent of total deaths, and death rates for the 15 leading causes of death in selected age groups, by race and Hispanic origin, and sex: United States, 2016. (https://www.cdc.gov/nchs/data/dvs/lcwk/lcwk3_hr_2016.pdf).
-
- Hennekens CH, Dyken ML, Fuster V. Aspirin as a therapeutic agent in cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation 1997; 96: 2751–3. - PubMed
-
- Ajani UA, Ford ES, Greenland KJ, Giles WH, Mokdad AH. Aspirin use among U.S. adults: Behavioral Risk Factor Surveillance System. Am J Prev Med 2006; 30:7 4–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical