

Impact of sex hormones on immune function and multiple sclerosis development
- PMID: 30222193
- PMCID: PMC6283654
- DOI: 10.1111/imm.13004
Impact of sex hormones on immune function and multiple sclerosis development
Abstract
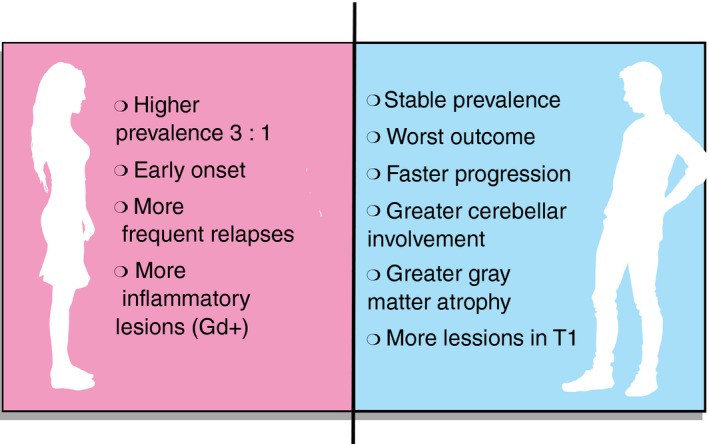
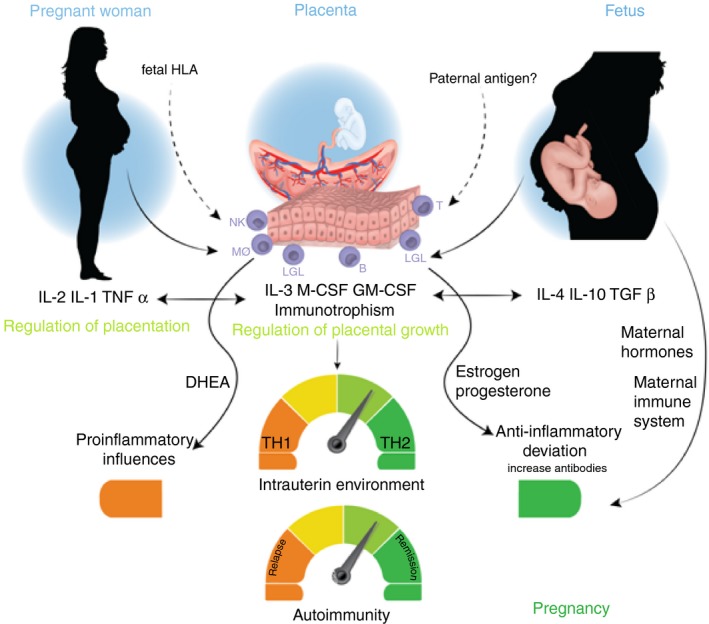
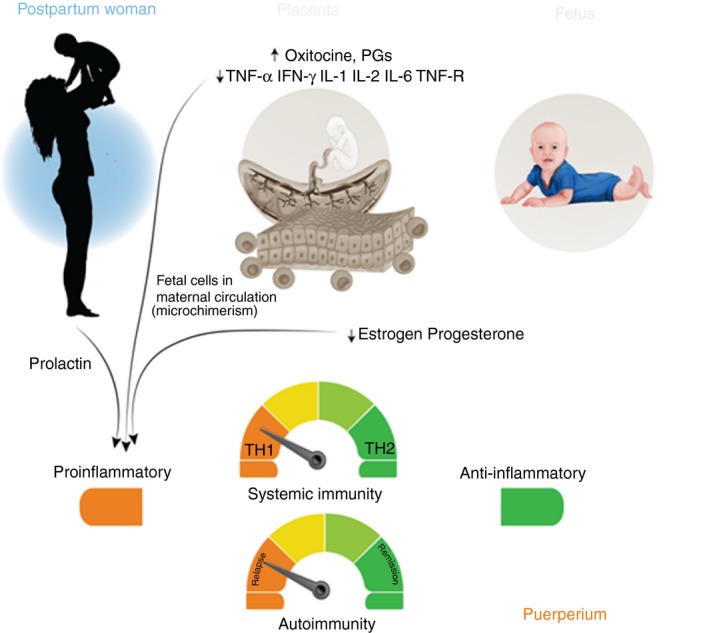
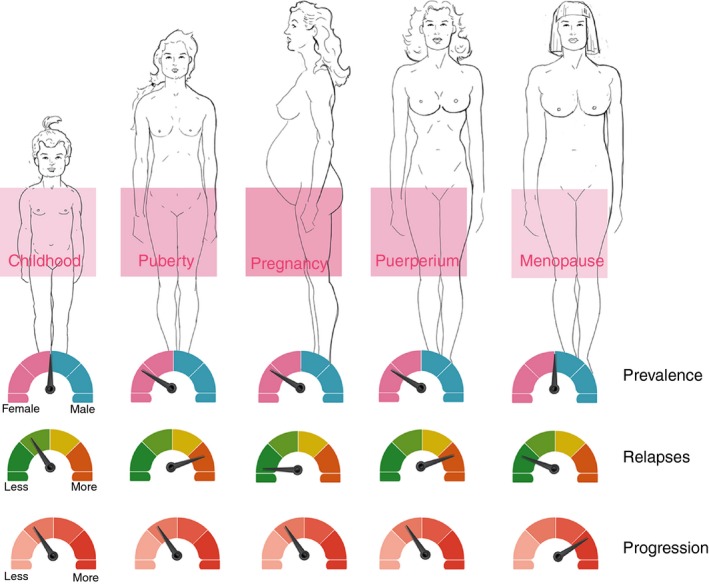
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system (CNS) affecting young people and leading to demyelination and neurodegeneration. The disease is clearly more common in women, in whom incidence has been rising. Gender differences include: earlier disease onset and more frequent relapses in women; and faster progression and worse outcomes in men. Hormone-related physiological conditions in women such as puberty, pregnancy, puerperium, and menopause also exert significant influence both on disease prevalence as well as on outcomes. Hormonal and/or genetic factors are therefore believed to be involved in regulating the course of disease. In this review, we discuss clinical evidence for the impact of sex hormones (estrogens, progesterone, prolactin, and testosterone) on MS and attempt to elucidate the hormonal and immunological mechanisms potentially underlying these changes. We also review current knowledge on the relationship between sex hormones and resident CNS cells and provide new insights in the context of MS. Understanding these molecular mechanisms may contribute to the development of new and safer treatments for both men and women.
Keywords: gender; multiple sclerosis; pregnancy; sex hormones.
© 2018 John Wiley & Sons Ltd.
Figures
References
-
- Koch‐Henriksen N, Sørensen PS. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol 2010; 9:520–32. - PubMed
-
- Confavreux C, Aimard G, Devic M. Course and prognosis of multiple sclerosis assessed by the computerized data processing of 349 patients. Brain 1980; 103:281–300. - PubMed
-
- Orton S‐M, Herrera BM, Yee IM, Valdar W, Ramagopalan SV, Sadovnick AD et al Sex ratio of multiple sclerosis in Canada: a longitudinal study. Lancet Neurol 2006; 5:932–6. - PubMed
-
- Ramagopalan SV, Byrnes JK, Orton S‐MS‐M, Dyment DA, Guimond C, Yee IM et al Sex ratio of multiple sclerosis and clinical phenotype. Eur J Neurol 2010; 17:634–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
