

Rapidly Progressive Dementia in the Outpatient Clinic: More Than Prions
- PMID: 30222606
- PMCID: PMC6249048
- DOI: 10.1097/WAD.0000000000000276
Rapidly Progressive Dementia in the Outpatient Clinic: More Than Prions
Abstract
Background: Published approaches to the evaluation and management of patients with rapidly progressive dementia (RPD) have been largely informed by experience at academic hospitals and national centers specializing in the diagnosis of Creutzfeldt-Jakob disease. Whether these approaches can be applied to patients assessed within lower-acuity outpatient settings is unknown.
Methods: A total of 96 patients with suspected RPD were assessed within the Washington University School of Medicine (Saint Louis, MO) outpatient memory clinic from February 2006 to February 2016. Consensus etiologic diagnoses were established following independent review of clinical data by 2 dementia specialists.
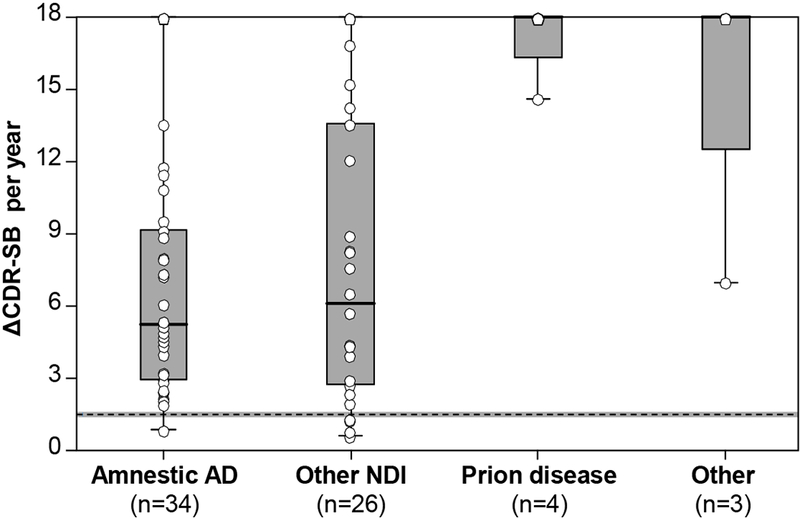
Results: In total, 67/90 (70%) patients manifested with faster-than-expected cognitive decline leading to dementia within 2 years of symptom onset. Female sex (42/67, 63%), median patient age (68.3 y; range, 45.4 to 89.6), and years of education (12 y; range, 6 to 14) were consistent with clinic demographics. Atypical presentations of common neurodegenerative dementing illnesses accounted for 90% (60/67) of RPD cases. Older age predicted a higher odds of amnestic Alzheimer disease dementia (OR, 2.1 per decade; 95% CI, 1.1-3.8; P=0.02). Parkinsonism (OR, 6.9; 95% CI, 1.6-30.5; P=0.01) or cortical visual dysfunction (OR, 10.8; 95% CI, 1.7-69.4; P=0.01) predicted higher odds of another neurodegenerative cause of RPD, including sporadic Creutzfeldt-Jakob disease.
Conclusions and relevance: The clinical environment influences the prevalence of RPD causes. The clinical evaluation should be adapted to promote detection of common causes of RPD, specific to the practice setting.
Figures
References
-
- Poser S, Mollenhauer B, Krauβ A, et al. How to improve the clinical diagnosis of Creutzfeldt–Jakob disease. Brain. 1999;122(12):2345–2351. - PubMed
-
- Papageorgiou SG, Kontaxis T, Bonakis A, Karahalios G, Kalfakis N, Vassilopoulos D. Rapidly progressive dementia: causes found in a Greek tertiary referral center in Athens. Alzheimer Dis Assoc Disord. 2009;23(4):337–346. - PubMed
-
- Sala I, Marquie M, Sanchez-Saudinos MB, et al. Rapidly progressive dementia: experience in a tertiary care medical center. Alzheimer Dis Assoc Disord. 2012;26(3):267–271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
