

Drug susceptibility testing of slowly growing non-tuberculous mycobacteria using slomyco test-system
- PMID: 30222736
- PMCID: PMC6141080
- DOI: 10.1371/journal.pone.0203108
Drug susceptibility testing of slowly growing non-tuberculous mycobacteria using slomyco test-system
Abstract
Objective: The objective of the research was to assess the susceptibility of the slowly growing nontuberculous mycobacteria strains to the antimicrobial drugs used for mycobaterioses treatment using SLOMYCO test system.
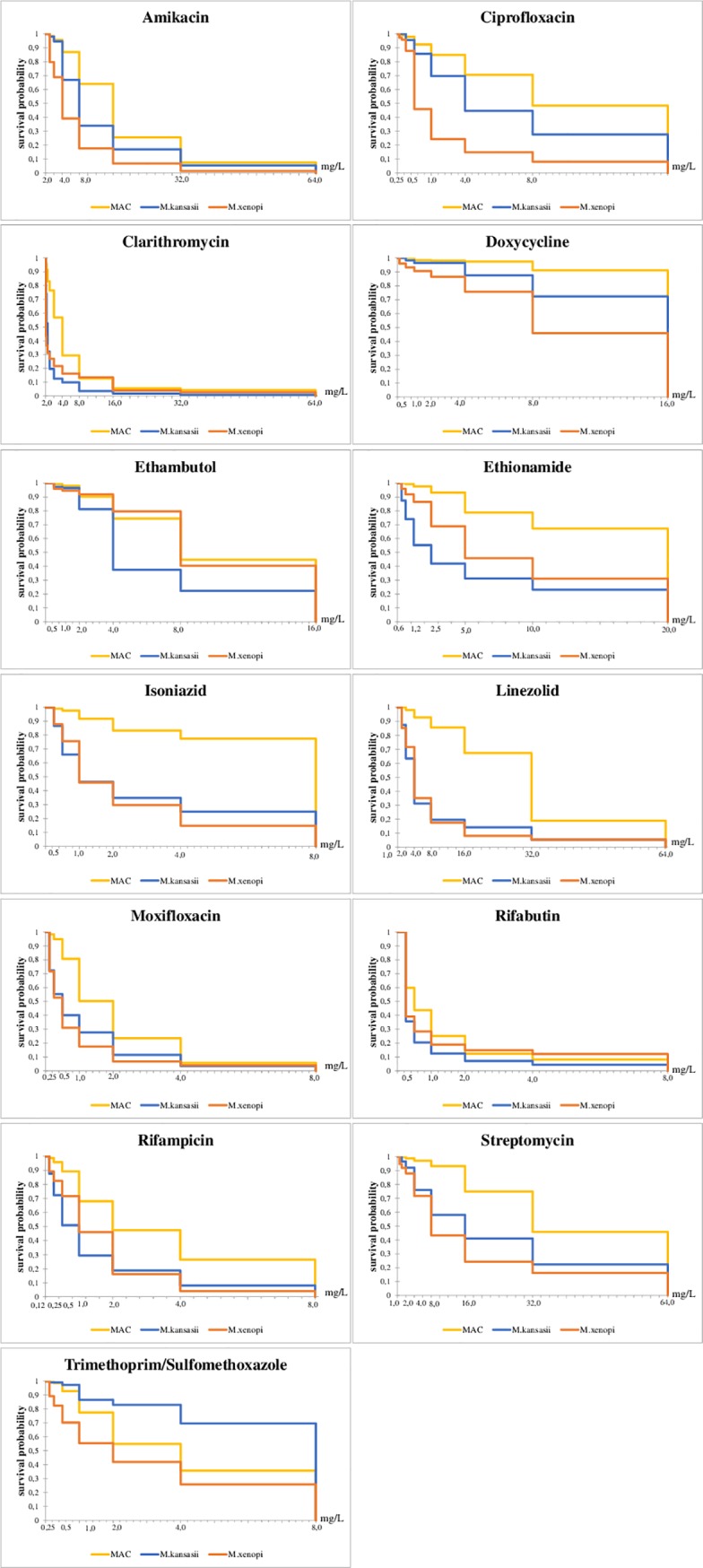
Materials and methods: We assessed 363 NTM strains: 177 MAC (161 M. avium, 16 M. intracellulare), 112 M. kansasii and 74 M. xenopi collected from the respiratory material of the patients were under the treatment or under diagnostic procedures at our Center, affiliates and the diagnostic department in 2010-2016. Drug sucseptibility for NTM was tested using the Sensititre SLOWMYCO system (TREK DIAGNOSTIC Systems Ltd., UK). MICs were established by microdilutions in Mueller-Hinton broth on polystyrene 96-well plates. The statistical analysis was done using the StatGraphics Plus 5.0 software. The data were compared pairwise using Pearson χ2 test with Yates correction. 95% confidence interval (CI) were calculated. Statistically significant differences were considered for p <0.05. Log-rank test and Kaplan-Meier curves were used to assess the concentration-dependent surveillance probability.
Results: The statistically significant differences were revealed in sensitivity/resistance isolates of M. avium and M. intracellulare: M. avium strains were resistant to higher concentrations of amikacin, clarithromycin, linezolid and streptomycin (p <0.01); M. intracellulare strains were resistant to higher concentrations of ethionamide (p <0.05). The isolates of M. avium were significantly more resistant than M. kansasii to amikacin, doxycycline, isoniazid, clarithromycin, linezolid, moxifloxacin, rifabutin, rifampicin, streptomycin, trimethoprim/sulfamethoxazole, ciprofloxacin, ethambutol, ethionamide (visible growth of M. avium were inhibited by higher drug concentrations, p <0.01). The isolates of M. avium showed significantly higher resistance than M. xenopi to amikacin, doxycycline, isoniazid, clarithromycin, linezolid, moxifloxacin, rifampicin, streptomycin, trimethoprim/sulfamethoxazole, ciprofloxacin, ethambutol, and ethionamide (visible growth of M. avium were inhibited by higher drug concentrations, p <0.01). Statistically significant differences in the dynamics of the response to the antibacterial effects of isoniazid, linezolid, moxifloxacin, rifampicin, trimethoprim/sulfamethoxazole, ethambutol, and ethionamide were found for M. intracellulare and M. xenopi (complete inhibition of the visible growth of M. intracellulare required higher drugs concentrations, p <0, 05). Comparison of the Kaplan-Meyer curves revealed statistically significant differences in survialence probability of M. kansasii and M. xenopi for amikacin, doxycycline, rifampicin, trimethoprim/sulfamethoxazole, ciprofloxacin, ethambutol, and ethionamide (a higher number of isolates of M. xenopi were inhibited by low drugs concentrations, p <0.05).
Conclusions: Our data show that M. avium and M. intracellulare were more resistant to the majority of the studied drugs than M. kansasii and M. xenopi.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Adle-Biassette H., Huerre M., Breton G., Ruimy R., Carbonnelle A., Trophilme D., et al. Nontuberculous mycobacterial diseases. Ann. Pathol. 2003; 23(3):216–235. - PubMed
-
- Otten T.F., Vasiliev A.V. Mycobacteriosis St. Petersburg: Med. Press;2005.
-
- Brown-Elliott B., Wallace R. Infections caused by nontuberculous mycobacteria. In: Principles and Practice of Infectious Disease. (eds. Mandell G.). 2005; 2: 2909–2916.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
