

Clinical molecular testing for ASXL1 c.1934dupG p.Gly646fs mutation in hematologic neoplasms in the NGS era
- PMID: 30222780
- PMCID: PMC6141087
- DOI: 10.1371/journal.pone.0204218
Clinical molecular testing for ASXL1 c.1934dupG p.Gly646fs mutation in hematologic neoplasms in the NGS era
Abstract
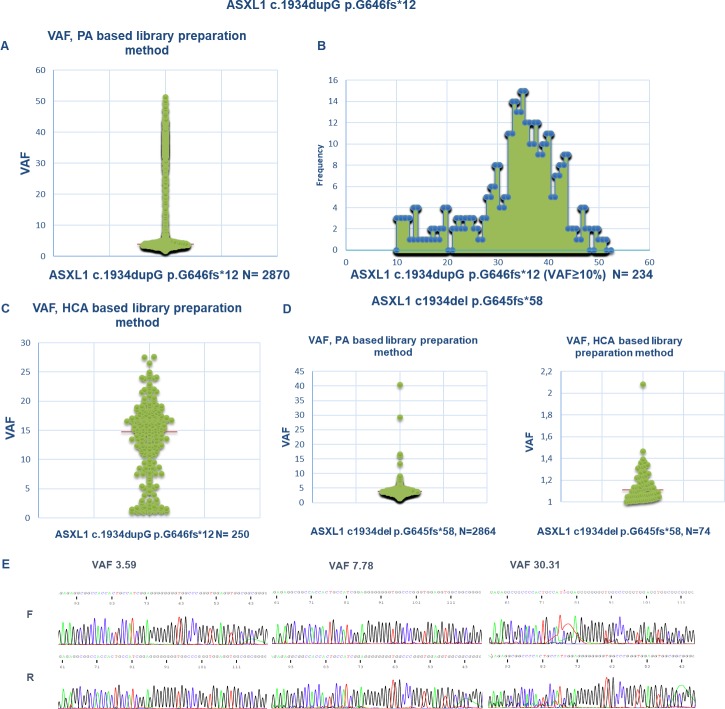
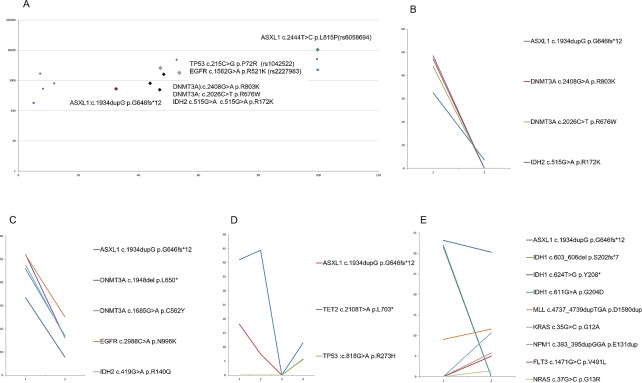
ASXL1 (additional sex combs like 1) is a gene that is mutated in a number of hematological neoplasms. The most common genetic alteration is c.1934dupG p.Gly646fs. Previous publications have shown that ASXL1 mutations have a negative prognostic impact in patients with MDS and AML, however, controversy exists regarding the molecular testing of ASXL1 c.1934dupG as polymerase splippage over the adjacent homopolymer could lead to a false-positive result. Here, we report the first study to systematically test different targeted next generation sequencing (NGS) approaches for this mutation in patients with hematologic neoplasms. In addition, we investigated the impact of proofreading capabilities of different DNA polymerases on ASXL1 c.1934dupG somatic mutation using conventional Sanger sequencing, another common method for ASXL1 genotyping. Our results confirm that ASXL1 c.1934dupG can be detected as a technical artifact, which can be overcome by the use of appropriate enzymes and library preparation methods. A systematic study of serial samples from 30 patients show that ASXL1 c.1934dupG is a somatic mutation in haematological neoplasms including MDS, AML, MPN and MDS/MPN and often is associated with somatic mutations of TET2, EZH2, IDH2, RUNX1, NRAS and DNMT3A. The pattern of clonal evolution suggests that this ASXL1 mutation might be an early mutational event that occurs in the principal clonal population and can serve as a clonal marker for persistent/relapsing disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
PCR-Fluo-ASXL1-FA: A fast, sensitive and inexpensive complementary method to detect ASXL1 mutations in haematological malignancies.Int J Lab Hematol. 2022 Oct;44(5):928-933. doi: 10.1111/ijlh.13931. Epub 2022 Jul 6. Int J Lab Hematol. 2022. PMID: 35793805
-
Discriminating a common somatic ASXL1 mutation (c.1934dup; p.G646Wfs*12) from artifact in myeloid malignancies using NGS.Leukemia. 2018 Aug;32(8):1874-1878. doi: 10.1038/s41375-018-0193-y. Epub 2018 Jun 29. Leukemia. 2018. PMID: 29959414 Free PMC article. No abstract available.
-
Routine clinical mutation profiling using next generation sequencing and a customized gene panel improves diagnostic precision in myeloid neoplasms.Oncotarget. 2016 May 24;7(21):30084-93. doi: 10.18632/oncotarget.8310. Oncotarget. 2016. PMID: 27029036 Free PMC article. Review.
-
Improved Variant Detection in Clinical Myeloid NGS Testing by Supplementing a Commercial Myeloid NGS Assay with Custom or Extended Data Filtering and Accessory Fragment Analysis.Mol Diagn Ther. 2021 Mar;25(2):251-266. doi: 10.1007/s40291-021-00519-5. Epub 2021 Mar 9. Mol Diagn Ther. 2021. PMID: 33687704
-
Genetic alterations crossing the borders of distinct hematopoetic lineages and solid tumors: Diagnostic challenges in the era of high-throughput sequencing in hemato-oncology.Crit Rev Oncol Hematol. 2018 Jun;126:64-79. doi: 10.1016/j.critrevonc.2018.03.020. Epub 2018 Mar 29. Crit Rev Oncol Hematol. 2018. PMID: 29759569 Review.
Cited by
-
[Clonal evolution of myelodysplastic syndrome].Zhonghua Xue Ye Xue Za Zhi. 2019 Dec 14;40(12):1060-1064. doi: 10.3760/cma.j.issn.0253-2727.2019.12.021. Zhonghua Xue Ye Xue Za Zhi. 2019. PMID: 32023745 Free PMC article. Chinese. No abstract available.
-
Prognostic impact of ASXL1 mutations in chronic phase chronic myeloid leukemia.Blood Cancer J. 2022 Oct 28;12(10):144. doi: 10.1038/s41408-022-00742-1. Blood Cancer J. 2022. PMID: 36307398 Free PMC article.
-
A reappraisal of ASXL1 mutation sites and the cohesin-binding motif in myeloid disease.Blood Cancer J. 2023 Jun 26;13(1):96. doi: 10.1038/s41408-023-00876-w. Blood Cancer J. 2023. PMID: 37365170 Free PMC article. No abstract available.
-
A practical approach to curate clonal hematopoiesis of indeterminate potential in human genetic data sets.Blood. 2023 May 4;141(18):2214-2223. doi: 10.1182/blood.2022018825. Blood. 2023. PMID: 36652671 Free PMC article.
-
Clinical implications of recurrent gene mutations in acute myeloid leukemia.Exp Hematol Oncol. 2020 Mar 27;9:4. doi: 10.1186/s40164-020-00161-7. eCollection 2020. Exp Hematol Oncol. 2020. PMID: 32231866 Free PMC article. Review.
References
-
- Pratcorona M, Abbas S, Sanders MA, Koenders JE, Kavelaars FG, Erpelinck-Verschueren CA, et al. Acquired mutations in ASXL1 in acute myeloid leukemia: prevalence and prognostic value. Haematologica. 2012;97(3):388–92. 10.3324/haematol.2011.051532 ; PubMed Central PMCID: PMCPMC3291593. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
