

Refractory juvenile myoclonic epilepsy: a meta-analysis of prevalence and risk factors
- PMID: 30223294
- PMCID: PMC6586162
- DOI: 10.1111/ene.13811
Refractory juvenile myoclonic epilepsy: a meta-analysis of prevalence and risk factors
Abstract
Background and purpose: Juvenile myoclonic epilepsy (JME) is a common epilepsy syndrome for which treatment response is generally assumed to be good. We aimed to determine the prevalence and prognostic risk factors for refractoriness of JME.
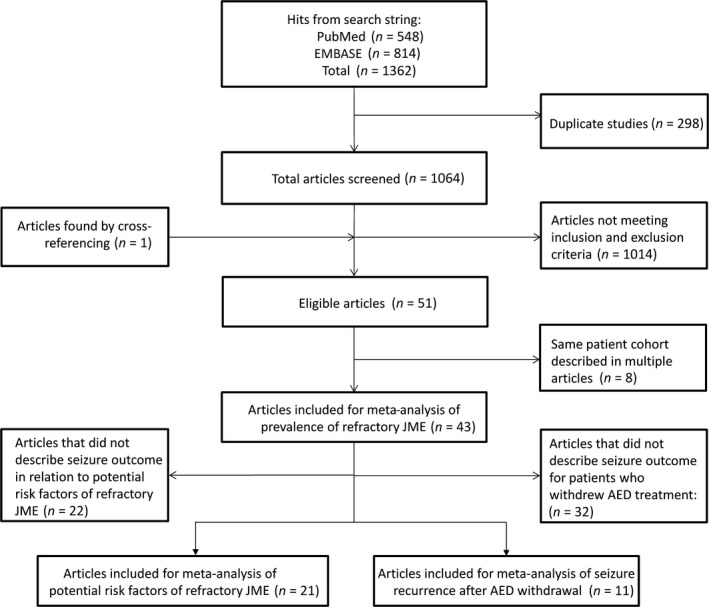
Methods: We systematically searched PubMed and EMBASE and included 43 eligible studies, reporting seizure outcome after antiepileptic drug (AED) treatment in JME cohorts. We defined refractory JME as persistence of any seizure despite AED treatment and performed a random-effects meta-analysis to assess the prevalence of refractory JME and of seizure recurrence after AED withdrawal in individuals with well-controlled seizures. Studies reporting potential prognostic risk factors in relation to seizure outcome were included for subsequent meta-analysis of risk factors for refractoriness.
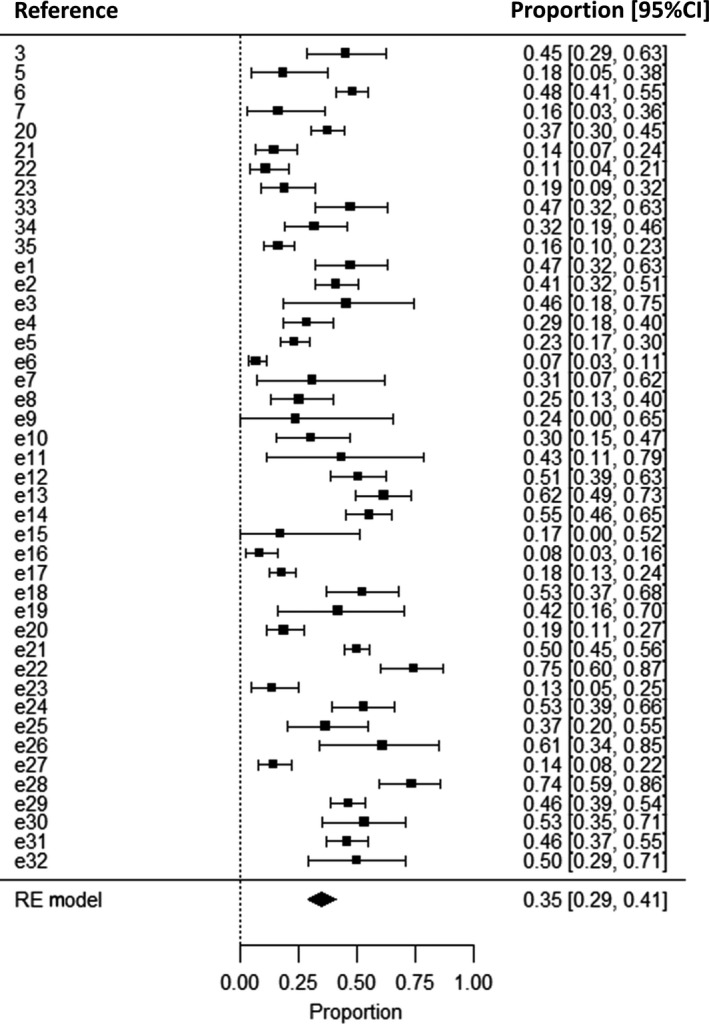
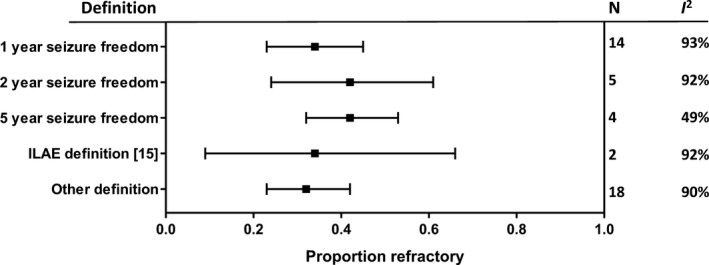
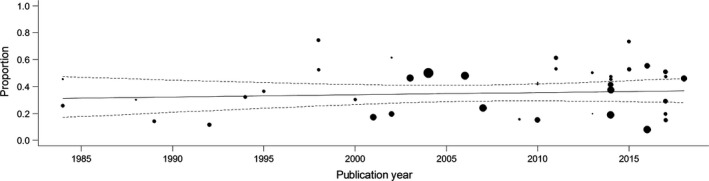
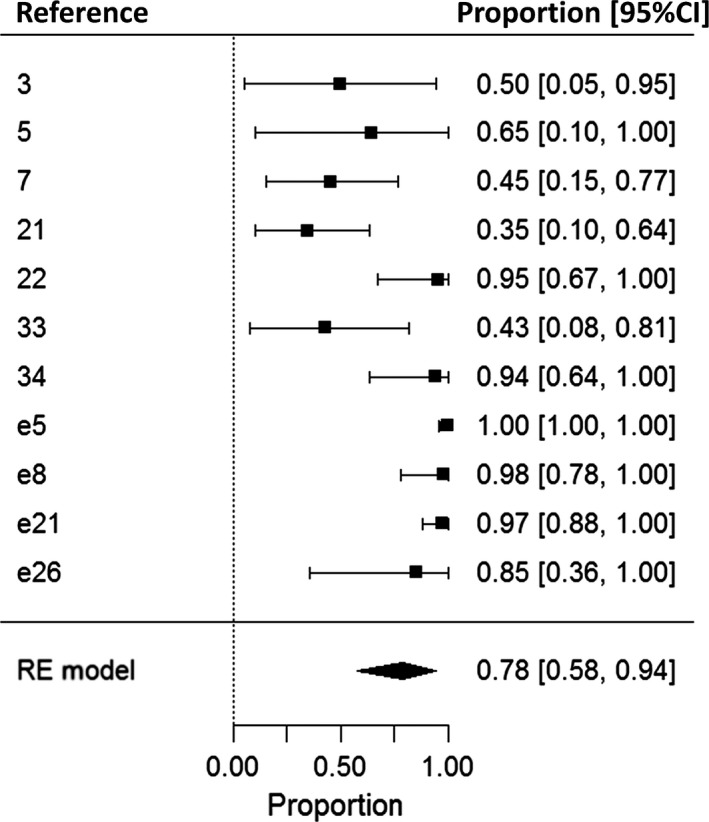
Results: Overall, 35% (95% confidence interval, 29-41%) of individuals (n = 3311) were refractory. There was marked heterogeneity between studies. Seizures recurred in 78% (95% confidence interval, 52-94%) of individuals who attempted to withdraw from treatment after a period of seizure freedom (n = 246). Seizure outcome by publication year suggested that prognosis did not improve over time. Meta-analysis suggested six variables as prognostic factors for refractoriness, i.e. having three seizure types, absence seizures, psychiatric comorbidities, earlier age at seizure onset, history of childhood absence epilepsy and praxis-induced seizures.
Conclusion: One-third of people with JME were refractory, which is a higher prevalence than expected. Risk factors were identified and can be used to guide treatment and counselling of people with JME.
Keywords: Janz syndrome; epilepsy; meta-analysis; pharmacoresistance; systematic review.
© 2018 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
The authors declare no financial or other conflicts of interest. J.W.S. reports grants and personal fees from Eisai, grants and personal fees from UCB, grants from WHO, grants from NEF, personal fees from Eisai, and grants and personal fees from UCB, outside the submitted work. His current position is endowed by the Epilepsy Society and he is a member of the Editorial Board of the
Figures
References
-
- Camfield CS, Striano P, Camfield PR. Epidemiology of juvenile myoclonic epilepsy. Epilepsy Behav 2013; 28(Suppl. 1): S15–S17. - PubMed
-
- Commission on Classification and Terminology of the International League Against Epilepsy . Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989; 30: 389–399. - PubMed
-
- Schneider‐von Podewils F, Gasse C, Geithner J, et al Clinical predictors of the long‐term social outcome and quality of life in juvenile myoclonic epilepsy: 20‐65 years of follow‐up. Epilepsia 2014; 55: 322–330. - PubMed
-
- Leidy NK, Elixhauser A, Vickrey B, Means E, Willian MK. Seizure frequency and the health‐related quality of life of adults with epilepsy. Neurology 1999; 53: 162–166. - PubMed
-
- Calleja S, Salas‐Puig J, Ribacoba R, Lahoz CH. Evolution of juvenile myoclonic epilepsy treated from the outset with sodium valproate. Seizure 2001; 10: 424–427. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
