Study of liver in HBV-related hepatocellular carcinoma: Stereology shows quantitative differences in liver structure
- PMID: 30223640
- PMCID: PMC6166574
- DOI: 10.4081/ejh.2018.2950
Study of liver in HBV-related hepatocellular carcinoma: Stereology shows quantitative differences in liver structure
Abstract
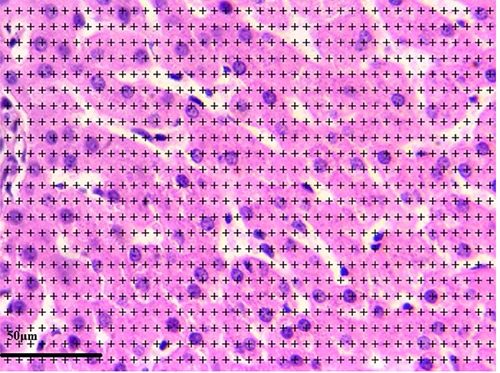
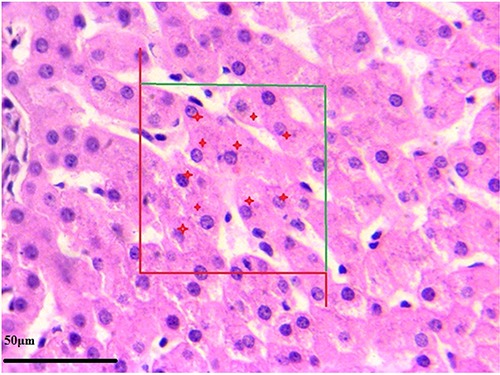
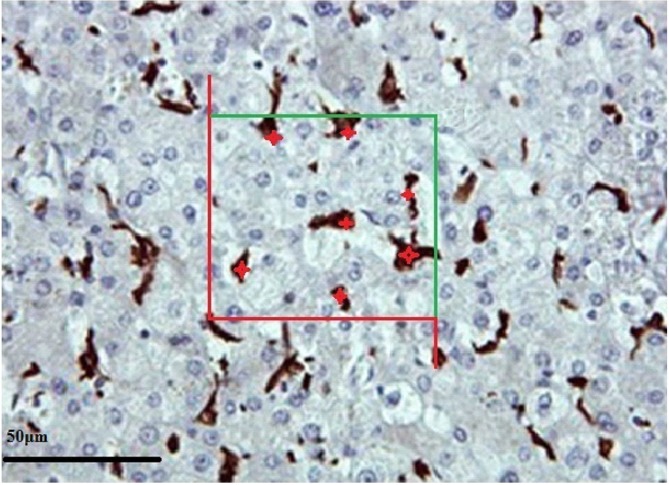
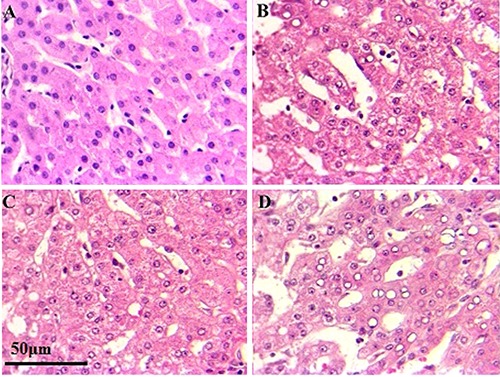
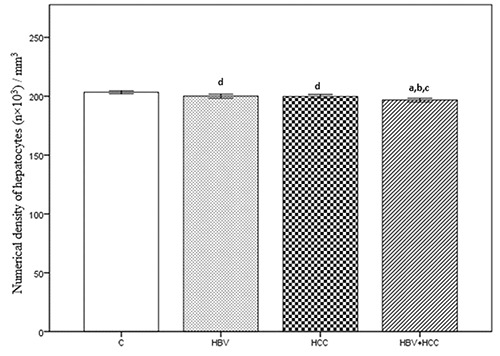
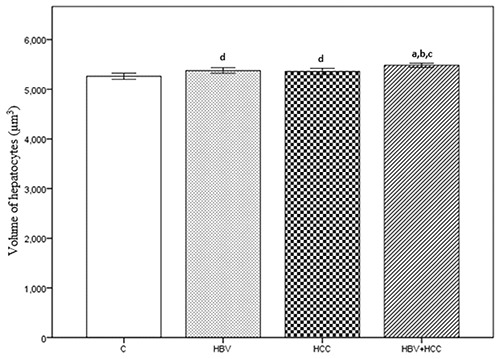
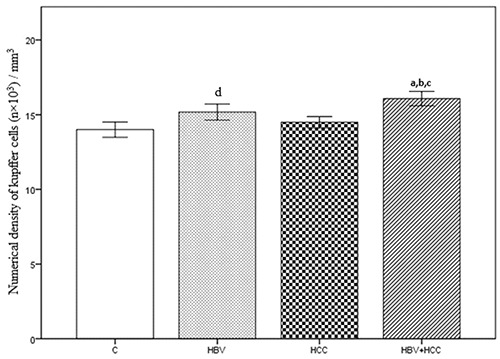
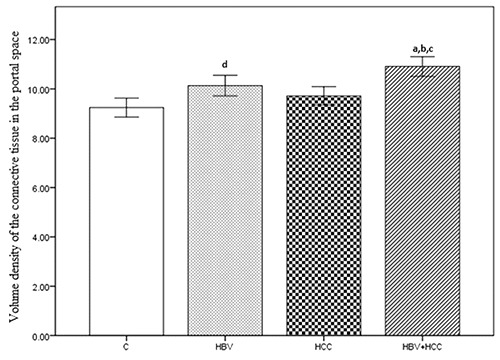
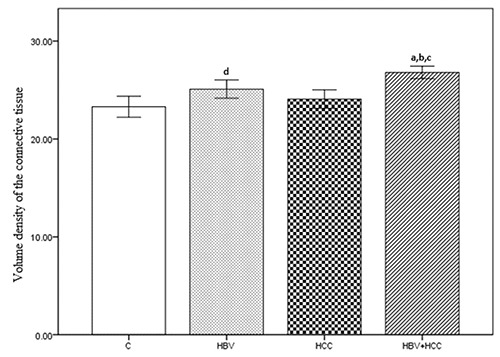
Hepatocellular carcinoma is one of the main consequences of liver chronic disease. Hepatocellular carcinoma-related changes may be seen in patients with chronic hepatitis B. The aim of the current study was to quantitate liver tissue elements by stereological technique in patients with hepatitis B-related cancer and compare the results with control and only hepatitis B group. Needle liver biopsies from 40 patients with only chronic hepatitis B infection, from 41 patients with only early hepatocellular carcinoma, from 40 patients with early hepatitis B-related cancer and 30 healthy subjects (control group) were analyzed by stereological method using systematic uniform random sampling method. Haematoxylin and eosin stained sections were used. The numerical density of hepatocytes, hepatocyte volume, numerical density of Kupffer cells, volume density of the connective tissue in the portal space, and volume density of the connective tissue were assessed. Quantitative analysis of liver samples indicated that there were statistically significant differences in the numerical density of hepatocytes, hepatocyte volume, numerical density of Kupffer cells, volume density of the connective tissue in the portal space, and volume density of the connective tissue between control and hepatitis B-related cancer and hepatitis B groups. Quantitative, stereological technique is simple and reliable for evaluating HCC in chronic hepatitis B. It is useful for assessing the liver tissue parameters. Stereology is recommended for the diagnosis of people prone to cancer in patients with chronic hepatitis B.
Conflict of interest statement
Conflict of interest: The Authors declare no conflict of interest.
Figures
Similar articles
-
Type II ground-glass hepatocytes as a marker of hepatocellular carcinoma in chronic hepatitis B.Hum Pathol. 2013 Aug;44(8):1665-71. doi: 10.1016/j.humpath.2013.01.020. Epub 2013 Apr 8. Hum Pathol. 2013. PMID: 23574780
-
Clonal expansion of hepatocytes with a selective advantage occurs during all stages of chronic hepatitis B virus infection.J Viral Hepat. 2015 Sep;22(9):737-53. doi: 10.1111/jvh.12380. Epub 2015 Jan 26. J Viral Hepat. 2015. PMID: 25619231
-
Resistance of ground glass hepatocytes to oral antivirals in chronic hepatitis B patients and implication for the development of hepatocellular carcinoma.Oncotarget. 2016 May 10;7(19):27724-34. doi: 10.18632/oncotarget.8388. Oncotarget. 2016. PMID: 27027237 Free PMC article.
-
Conceptual models for the initiation of hepatitis B virus-associated hepatocellular carcinoma.Liver Int. 2015 Jul;35(7):1786-800. doi: 10.1111/liv.12773. Epub 2015 Feb 9. Liver Int. 2015. PMID: 25640596 Review.
-
Direct effects of hepatitis B virus-encoded proteins and chronic infection in liver cancer development.Dig Dis. 2013;31(1):138-51. doi: 10.1159/000347209. Epub 2013 Jun 17. Dig Dis. 2013. PMID: 23797136 Review.
Cited by
-
Meta-analysis and systematic review of prognostic significance of Glypican-3 in patients with hepatitis B-related hepatocellular carcinoma.Virusdisease. 2019 Jun;30(2):193-200. doi: 10.1007/s13337-019-00517-6. Epub 2019 Mar 28. Virusdisease. 2019. PMID: 31179356 Free PMC article.
-
Stereological Evaluation of Rabbit Fetus Liver after Xenotransplantation of Human Wharton's Jelly-Derived Mesenchymal Stromal Cells.Int J Organ Transplant Med. 2022;13(1):15-24. Int J Organ Transplant Med. 2022. PMID: 37383424 Free PMC article.
-
Bi-Functional Peptides as a New Therapeutic Tool for Hepatocellular Carcinoma.Pharmaceutics. 2021 Oct 6;13(10):1631. doi: 10.3390/pharmaceutics13101631. Pharmaceutics. 2021. PMID: 34683924 Free PMC article.
-
Hepatocyte paraffin 1 and arginase-1 are effective panel of markers in HBV-related HCC diagnosis in fine-needle aspiration specimens.BMC Res Notes. 2020 Aug 20;13(1):388. doi: 10.1186/s13104-020-05230-y. BMC Res Notes. 2020. PMID: 32854754 Free PMC article.
References
-
- Ferenci P, Fried M, Labrecque D, Bruix J, Sherman M, Omata M, et al. World Gastroenterology Organisation Guideline. Hepatocellular carcinoma (HCC): a global perspective. J Gastroint Liver D 2010;19:311-7. - PubMed
-
- El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 2007;132:2557-76. - PubMed
-
- Moudi B, Heidari Z, Mahmoudzadeh -Sagheb H. Impact of host gene polymorphisms on susceptibility to chronic hepatitis B virus infection. Infect Genet Evol 2016;44:94-105. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical