

The Pathological Features of Colorectal Cancer Determine the Detection Performance on Blood ctDNA
- PMID: 30223720
- PMCID: PMC6144579
- DOI: 10.1177/1533033818791794
The Pathological Features of Colorectal Cancer Determine the Detection Performance on Blood ctDNA
Abstract
Background and aim: Methylated SEPT9 is a novel circulating tumor DNA marker for colorectal cancer, while the effects of various colorectal cancer clinicopathological factors on its detection performance have not been fully evaluated. This study aims to investigate the significance of the clinicopathological factors on methylated SEPT9 performance in a symptomatic endoscopy cohort, with a specific focus on colorectal cancer.
Methods: A total of 1160 participants were recruited in this study, including 300 patients with colorectal cancer, 122 patients with adenoma, 103 patients with hyperplastic polyps, 568 normal participants (no evidence of disease), and 67 patients with other gastrointestinal diseases. Peripheral blood samples of these participants were collected from 3 Chinese hospitals, and the methylated SEPT9 level was measured using the Epi proColon 2.0 assay.
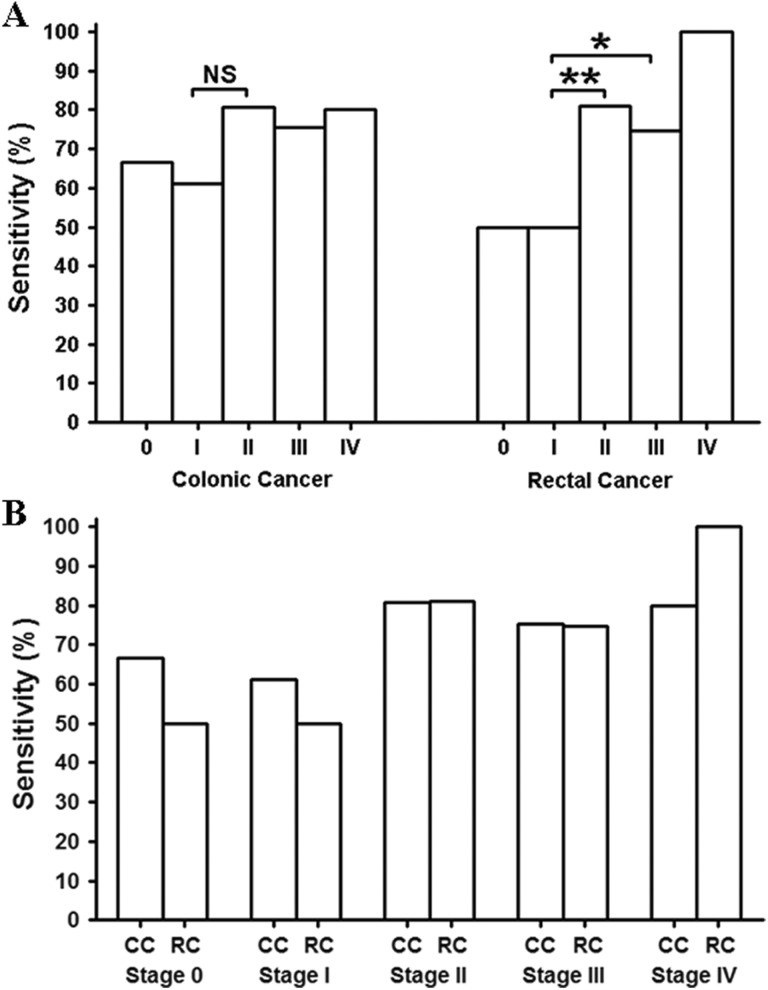
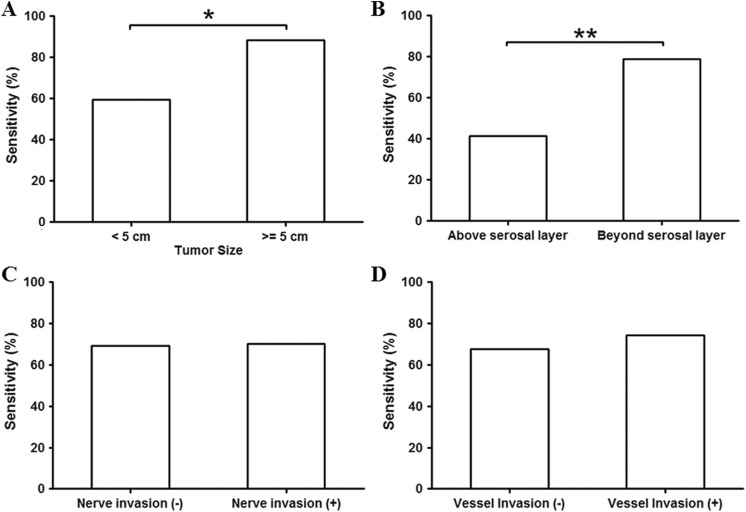
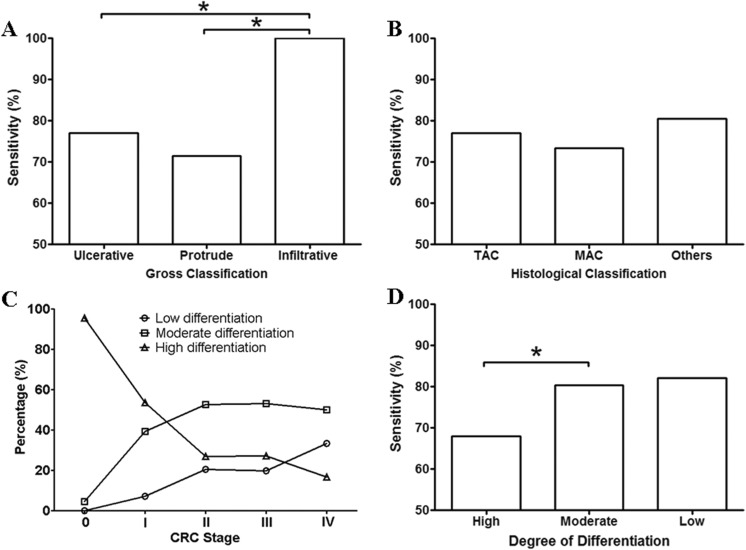
Results: Cancer stage, size, and invasion depth were positively correlated with the detection sensitivity, while no difference in sensitivity was identified among cancers at various locations. Infiltrative colorectal cancer exhibited higher sensitivity than ulcerative and protrude colorectal cancer, while no difference in sensitivity was observed among assessed histological types. The colorectal cancer differentiation showed a clear correlation with the cancer stage, and moderate and poorly differentiated colorectal cancer exhibited higher sensitivity than well-differentiated colorectal cancer. Furthermore, colorectal cancer with distal metastasis (M1) showed higher sensitivity than those without any metastasis, while colorectal cancer with lymph node metastasis (N1 and N2) did not show statistical significance compared to those without it. Finally, local vessel or nerve invasion did not affect the sensitivity.
Conclusion: Factors that reflect the colorectal cancer intrinsic properties, including cancer stage, size, invasion depth, classification, differentiation, and metastasis, exhibited significant effect on the mSEPT9 detection performance.
Keywords: SEPT9; adenoma; colorectal cancer; methylation; polyps; septin 9.
Conflict of interest statement
Figures



References
-
- Schreuders EH, Ruco A, Rabeneck L, et al. Colorectal cancer screening: a global overview of existing programmes. Gut. 2015;64(10):1637–1649. - PubMed
-
- National Cancer Institute, PDQ, Treatment, Health Professionals. Survival Rate for Colorectal Cancer by Stage. Bethesda, MD: National Cancer Institute; 1999.
-
- Lofton-Day C, Model F, Devos T, et al. DNA methylation biomarkers for blood-based colorectal cancer screening. Clin Chem. 2008;54(2):414–423. - PubMed
-
- Song L, Li Y. SEPT9: a specific circulating biomarker for colorectal cancer. Adv Clin Chem. 2015;72:171–204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
