

HIV partner services in Kenya: a cost and budget impact analysis study
- PMID: 30223833
- PMCID: PMC6142360
- DOI: 10.1186/s12913-018-3530-y
HIV partner services in Kenya: a cost and budget impact analysis study
Abstract
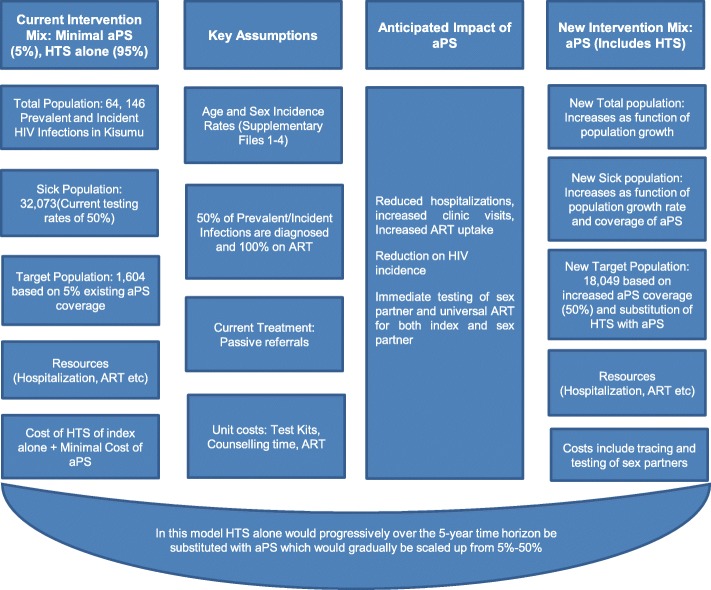
Background: The elicitation of contact information, notification and testing of sex partners of HIV infected patients (aPS), is an effective HIV testing strategy in low-income settings but may not necessarily be affordable. We applied WHO guidelines and the International Society for Pharmaco-economics and Outcomes Research (ISPOR) guidelines to conduct cost and budget impact analyses, respectively, of aPS compared to current practice of HIV testing services (HTS) in Kisumu County, Kenya.
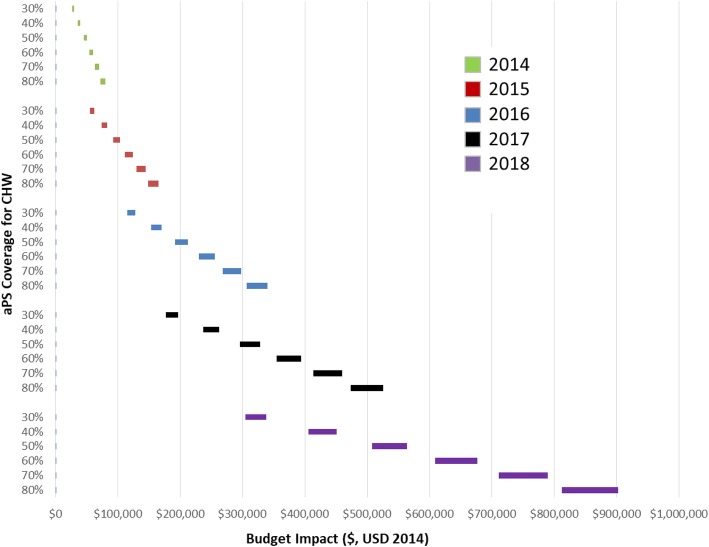
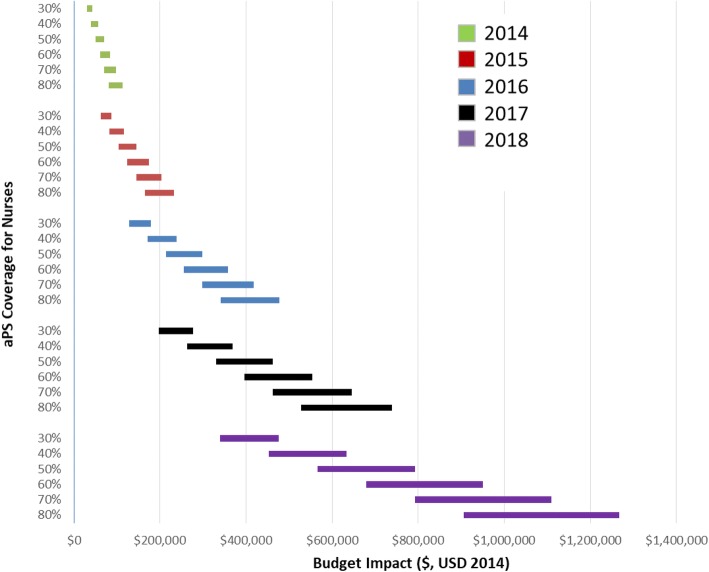
Methods: Using study data and time motion studies, we constructed an Excel-based tool to estimate costs and the budget impact of aPS. Cost data were collected from selected facilities in Kisumu County. We report the annual total and unit costs of HTS, incremental total and unit costs for aPS, and the budget impact of scaling up aPS over a 5-year horizon. We also considered a task-shifted scenario that used community health workers (CHWs) rather than facility based health workers and conducted sensitivity analyses assuming different rates of scale up of aPS.
Results: The average unit costs for HIV testing among HIV-infected index clients was US$ 25.36 per client and US$ 17.86 per client using nurses and CHWs, respectively. The average incremental costs for providing enhanced aPS in Kisumu County were US$ 1,092,161 and US$ 753,547 per year, using nurses and CHWs, respectively. The average incremental cost of scaling up aPS over a five period was 45% higher when using nurses compared to using CHWs (US$ 5,460,837 and US$ 3,767,738 respectively). Over the five years, the upper-bound budget impact of nurse-model was US$ 1,767,863, 63% and 35% of which were accounted for by aPS costs and ART costs, respectively. The CHW model incurred an upper-bound incremental cost of US$ 1,258,854, which was 71.2% lower than the nurse-based model. The budget impact was sensitive to the level of aPS coverage and ranged from US$ 28,547 for 30% coverage using CHWs in 2014 to US$ 1,267,603 for 80% coverage using nurses in 2018.
Conclusion: Scaling aPS using nurses has minimal budget impact but not cost-saving over a five-year period. Targeting aPS to newly-diagnosed index cases and task-shifting to community health workers is recommended.
Keywords: Budget impact analysis; Cost; HIV assisted partner services; Kenya.
Conflict of interest statement
Ethics approval and consent to participate
We obtained a research ethical approval from the University of Washington (43628C) and the Kenyatta National Hospital (P523/10/2012) Institutional Review Boards and no individual consent was obtained as this was considered a public health initiative.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Henley C, Forgwei G, Welty T, Golden M, Adimora A, Shields R, et al. Scale-up and case-finding effectiveness of an HIV partner services program in Cameroon: an innovative HIV prevention intervention for developing countries. Sex Transm Dis. 2013;40(12):909–914. doi: 10.1097/OLQ.0000000000000032. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
