

Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea
- PMID: 30223852
- PMCID: PMC6142353
- DOI: 10.1186/s12936-018-2481-4
Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea
Abstract
Background: Malaria in Equatorial Guinea remains a major public health problem. The country is a holo-endemic area with a year-round transmission pattern. In 2016, the prevalence of malaria was 12.09% and malaria caused 15% of deaths among children under 5 years. In the Continental Region, 95.2% of malaria infections were Plasmodium falciparum, 9.5% Plasmodium vivax, and eight cases mixed infection in 2011. The main strategy for malaria control is quick and accurate diagnosis followed by effective treatment. Early and accurate diagnosis of malaria is essential for both effective disease management and malaria surveillance. The quality of malaria diagnosis is important in all settings, as misdiagnosis can result in significant morbidity and mortality. Microscopy and RDTs are the primary choices for diagnosing malaria in the field. However, false-negative results may delay treatment and increase the number of persons capable of infecting mosquitoes in the community. The present study analysed the performance of microscopy and RDTs, the two main techniques used in Equatorial Guinea for the diagnosis of malaria, compared to semi-nested multiplex PCR (SnM-PCR).
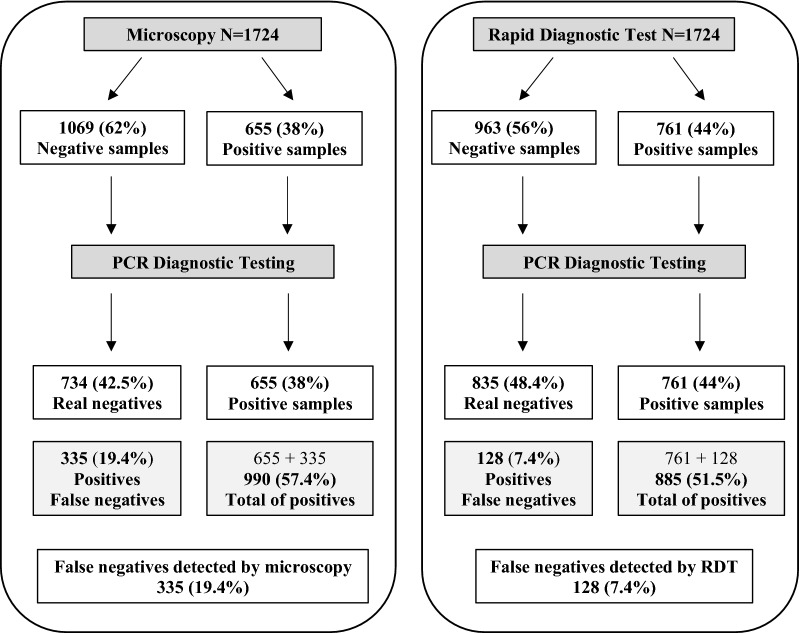
Results: A total of 1724 samples tested by microscopy, RDT, and SnM-PCR were analysed. Among the negative samples detected by microscopy, 335 (19.4%) were false negatives. On the other hand, the negative samples detected by RDT, 128 (13.3%) were false negatives based on PCR. This finding is important, especially since it is a group of patients who did not receive antimalarial treatment.
Conclusions: Owing to the high number of false negatives in microscopy, it is necessary to reinforce training in microscopy, the "Gold Standard" in endemic areas. A network of reference centres could potentially support ongoing diagnostic and control efforts made by malaria control programmes in the long term, as the National Centre of Tropical Medicine currently supports the National Programme against Malaria of Equatorial Guinea to perform all of the molecular studies necessary for disease control. Taking into account the results obtained with the RDTs, an exhaustive study of the deletion of the hrp2 gene must be done in EG to help choose the correct RDT for this area.
Keywords: Diagnosis; Malaria; Microscopy; RDTs; SnM-PCR.
Figures


References
-
- Benito A, Roche J, Molina R, Amela C, Alvar J. Application and evaluation of QBC malaria diagnosis in a holoendemic area. Appl Parasitol. 1994;35:266–272. - PubMed
-
- WHO . World malaria report 2017. Geneva: World Health Organization; 2017.
-
- Mendes C, Dias F, Figueiredo J, Mora VG, Cano J, de Sousa B, et al. Duffy negative antigen is no longer a barrier to Plasmodium vivax molecular evidences from the African West Coast (Angola and Equatorial Guinea) PLoS Negl Trop Dis. 2011;5:e1192. doi: 10.1371/journal.pntd.0001192. - DOI - PMC - PubMed
-
- Gerstl S, Dunkley S, Mukhtar A, De Smet M, Baker S, Maikere J. Assessment of two malaria rapid diagnostic tests in children under five years of age, with follow-up of false-positive pLDH test results, in a hyperendemic falciparum malaria area, Sierra Leone. Malar J. 2010;9:28. doi: 10.1186/1475-2875-9-28. - DOI - PMC - PubMed
-
- WHO . Guidelines for the treatment of malaria. Geneva: World Health Organization; 2010. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
