

NOTCH1 Represses MCL-1 Levels in GSI-resistant T-ALL, Making them Susceptible to ABT-263
- PMID: 30224339
- PMCID: PMC6320296
- DOI: 10.1158/1078-0432.CCR-18-0867
NOTCH1 Represses MCL-1 Levels in GSI-resistant T-ALL, Making them Susceptible to ABT-263
Abstract
Purpose: Effective targeted therapies are lacking for refractory and relapsed T-cell acute lymphoblastic leukemia (T-ALL). Suppression of the NOTCH pathway using gamma-secretase inhibitors (GSI) is toxic and clinically not effective. The goal of this study was to identify alternative therapeutic strategies for T-ALL.
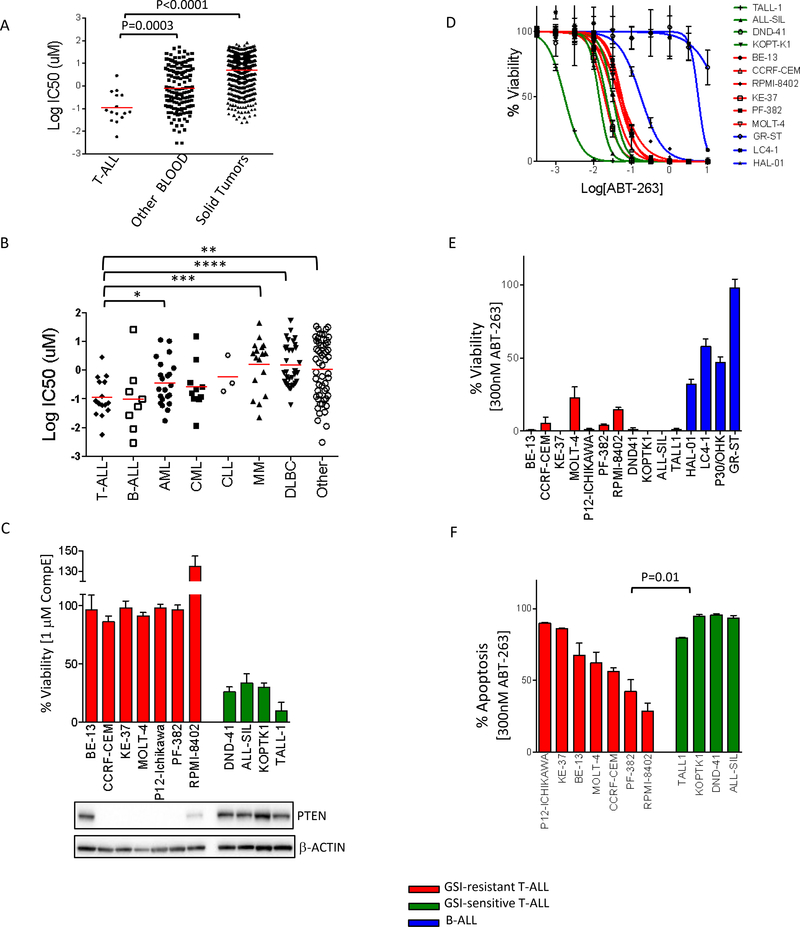
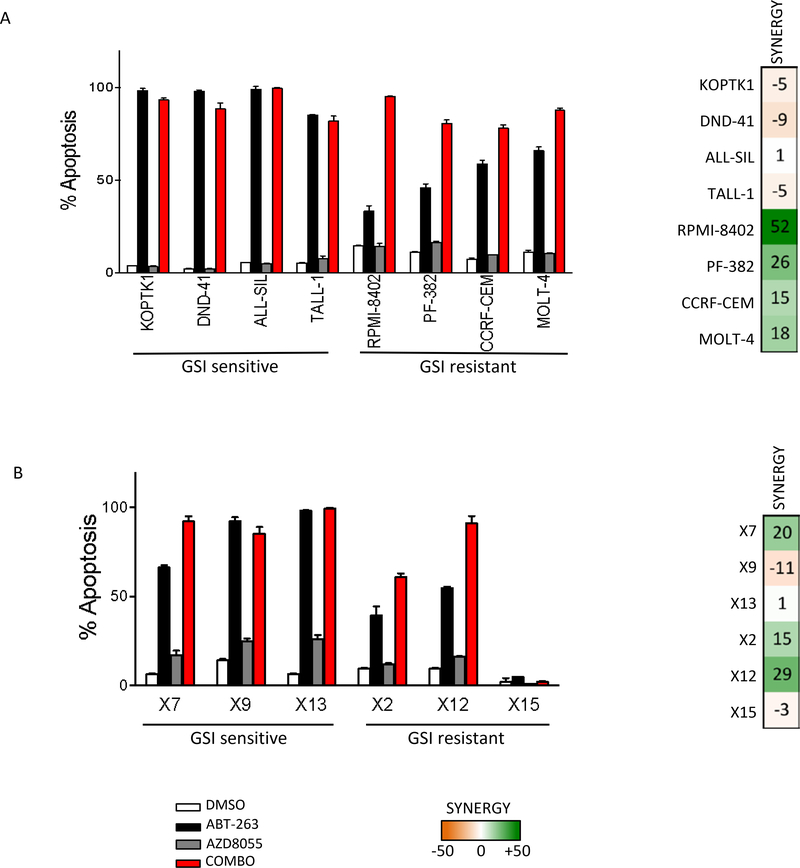
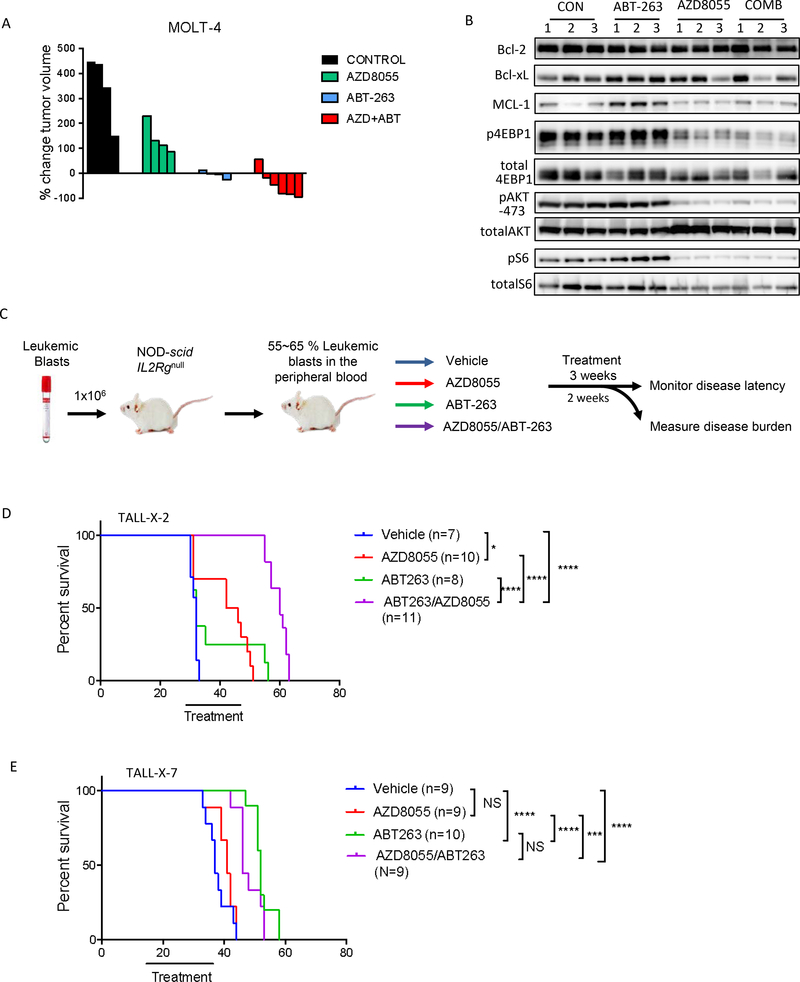
Experimental design: We performed a comprehensive analysis of our high-throughput drug screen across hundreds of human cell lines including 15 T-ALL models. We validated and further studied the top hit, navitoclax (ABT-263). We used multiple human T-ALL cell lines as well as primary patient samples, and performed both in vitro experiments and in vivo studies on patient-derived xenograft models.
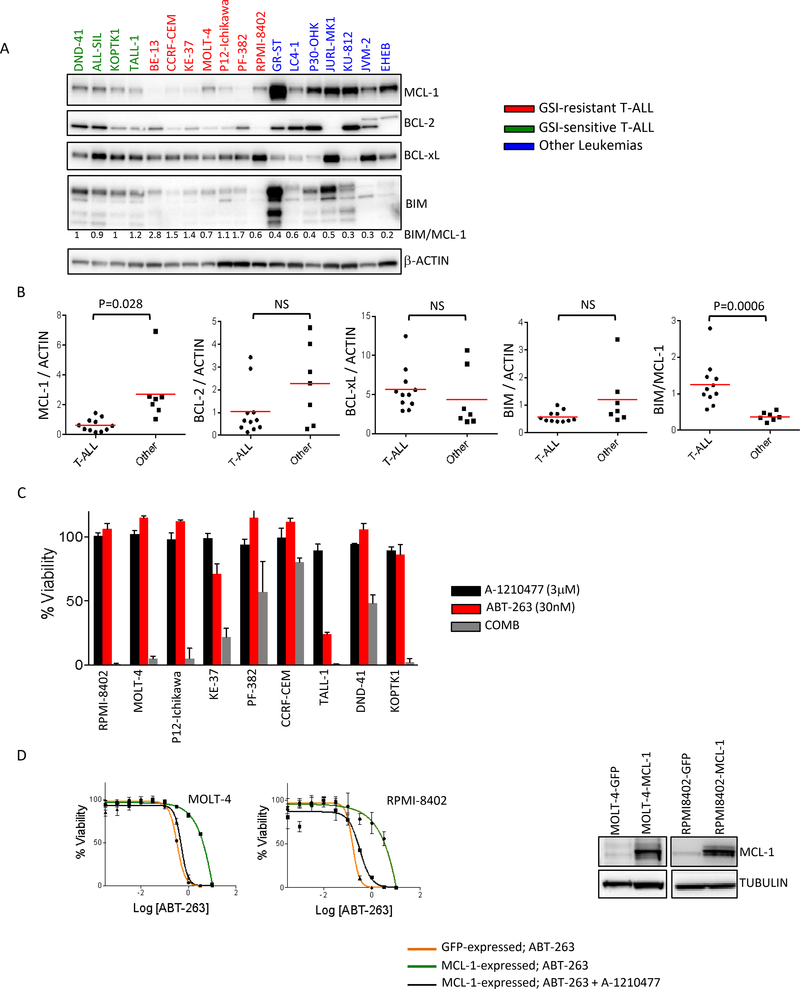
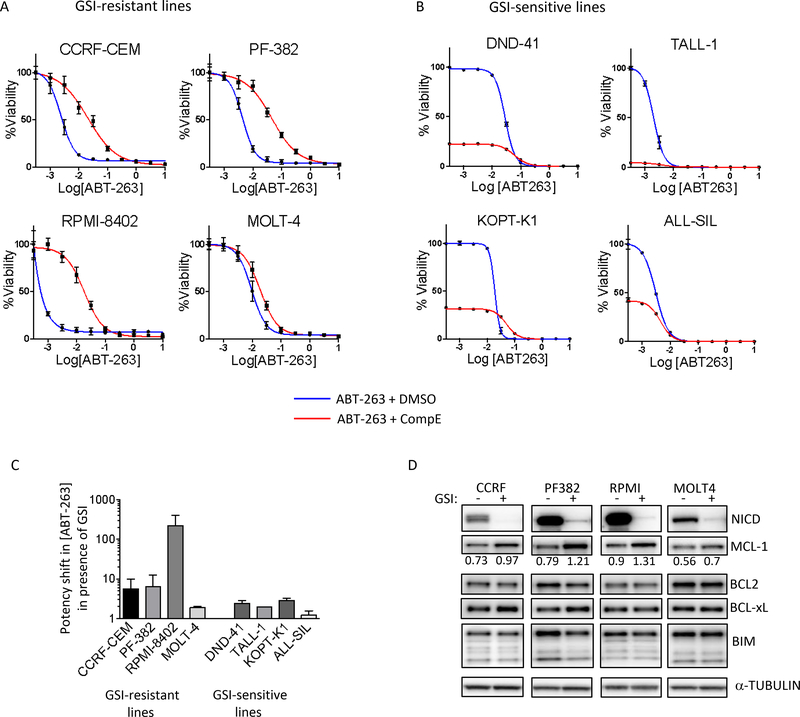
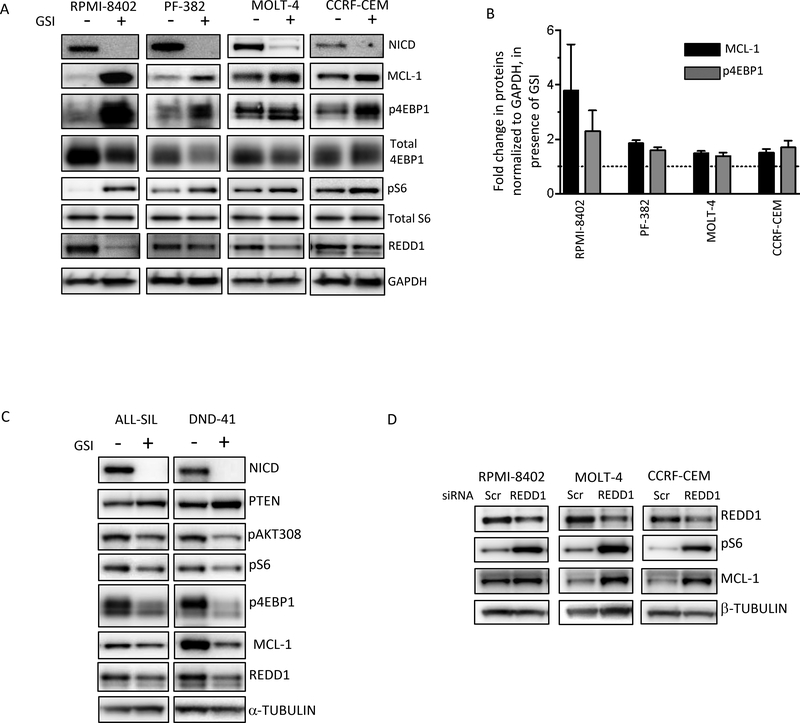
Results: We found that T-ALL are hypersensitive to navitoclax, an inhibitor of BCL2 family of antiapoptotic proteins. Importantly, GSI-resistant T-ALL are also susceptible to navitoclax. Sensitivity to navitoclax is due to low levels of MCL-1 in T-ALL. We identify an unsuspected regulation of mTORC1 by the NOTCH pathway, resulting in increased MCL-1 upon GSI treatment. Finally, we show that pharmacologic inhibition of mTORC1 lowers MCL-1 levels and further sensitizes cells to navitoclax in vitro and leads to tumor regressions in vivo.
Conclusions: Our results support the development of navitoclax, as single agent and in combination with mTOR inhibitors, as a new therapeutic strategy for T-ALL, including in the setting of GSI resistance.
©2018 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Ferrando AA, Neuberg DS, Staunton J, et al. Gene expression signatures define novel oncogenic pathways in T cell acute lymphoblastic leukemia. Cancer Cell. 2002;1(1):75–87. - PubMed
-
- Pui CH, Robison LL, Look AT. Acute lymphoblastic leukaemia. Lancet. 2008;371(9617):1030–1043. - PubMed
-
- Weng AP, Ferrando AA, Lee W, et al. Activating mutations of NOTCH1 in human T cell acute lymphoblastic leukemia. Science. 2004;306(5694):269–271. - PubMed
-
- Grabher C, von Boehmer H, Look AT. Notch 1 activation in the molecular pathogenesis of T-cell acute lymphoblastic leukaemia. Nat Rev Cancer. 2006;6(5):347–359. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
