

Sorafenib and Carfilzomib Synergistically Inhibit the Proliferation, Survival, and Metastasis of Hepatocellular Carcinoma
- PMID: 30224431
- PMCID: PMC9110113
- DOI: 10.1158/1535-7163.MCT-17-0541
Sorafenib and Carfilzomib Synergistically Inhibit the Proliferation, Survival, and Metastasis of Hepatocellular Carcinoma
Abstract
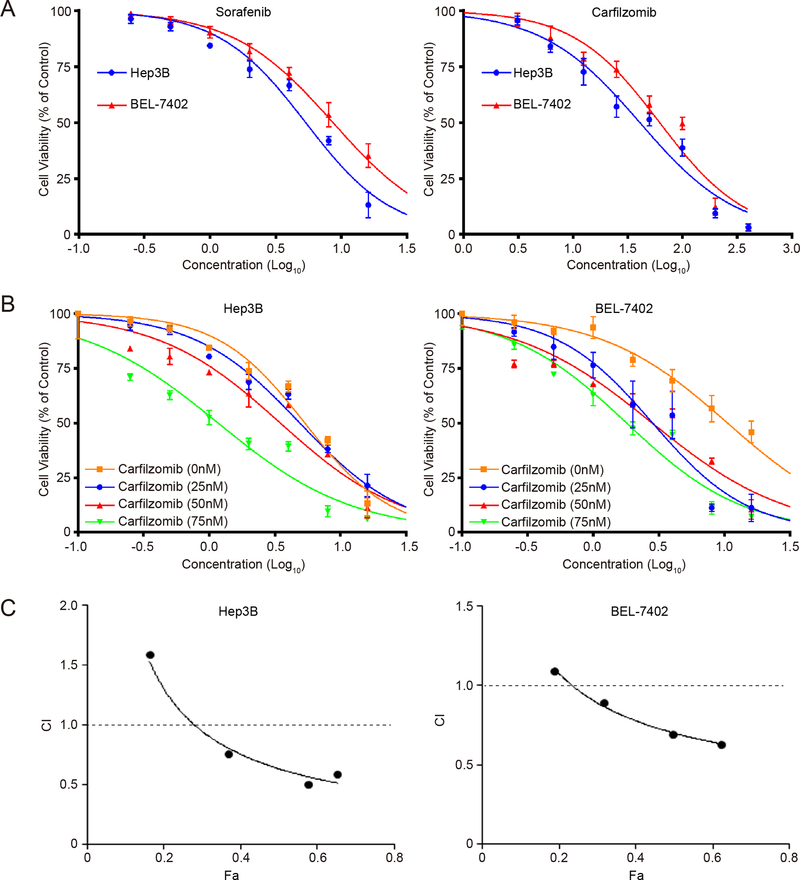
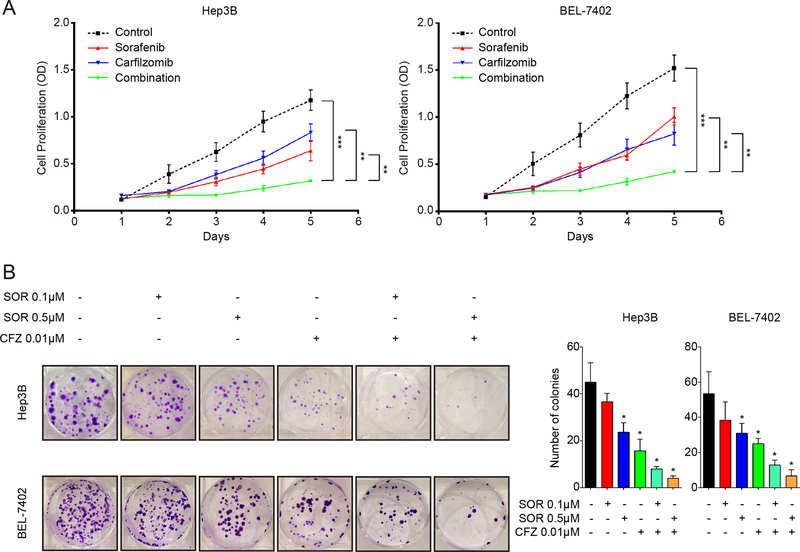
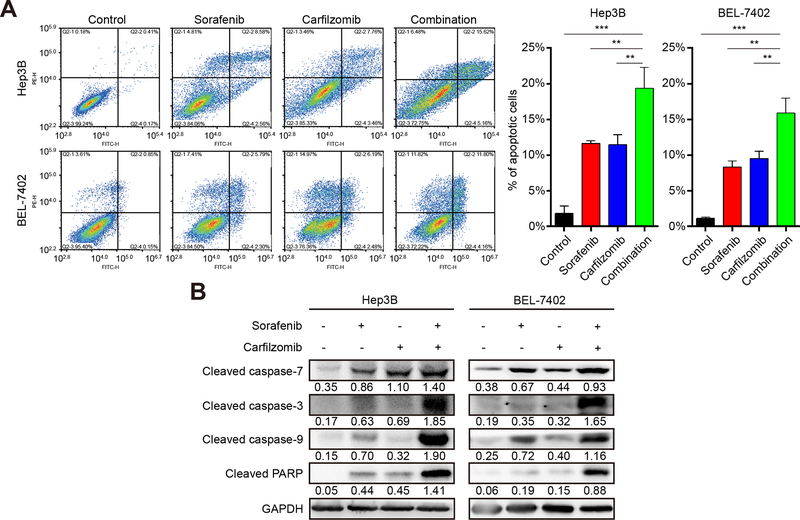
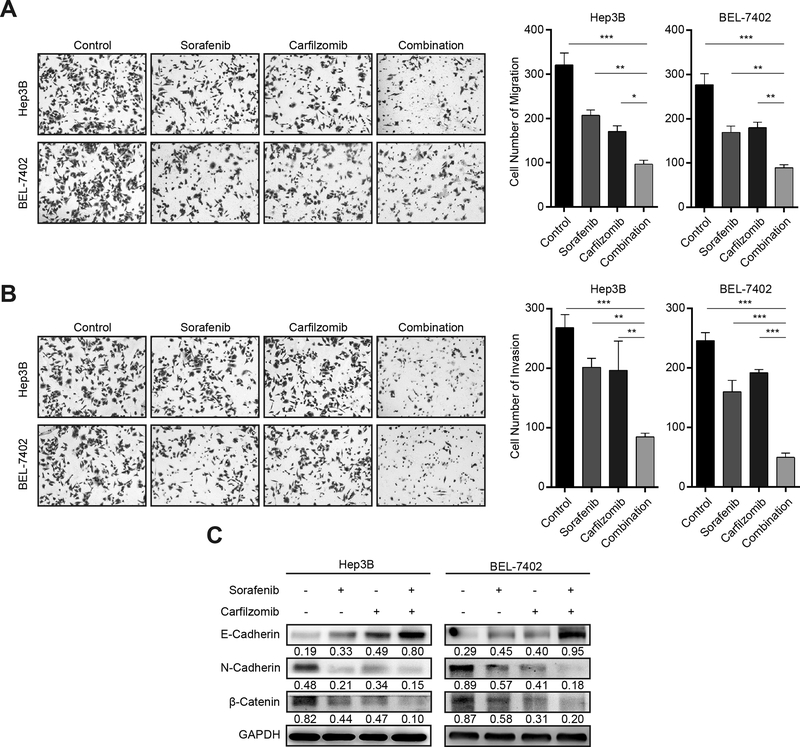
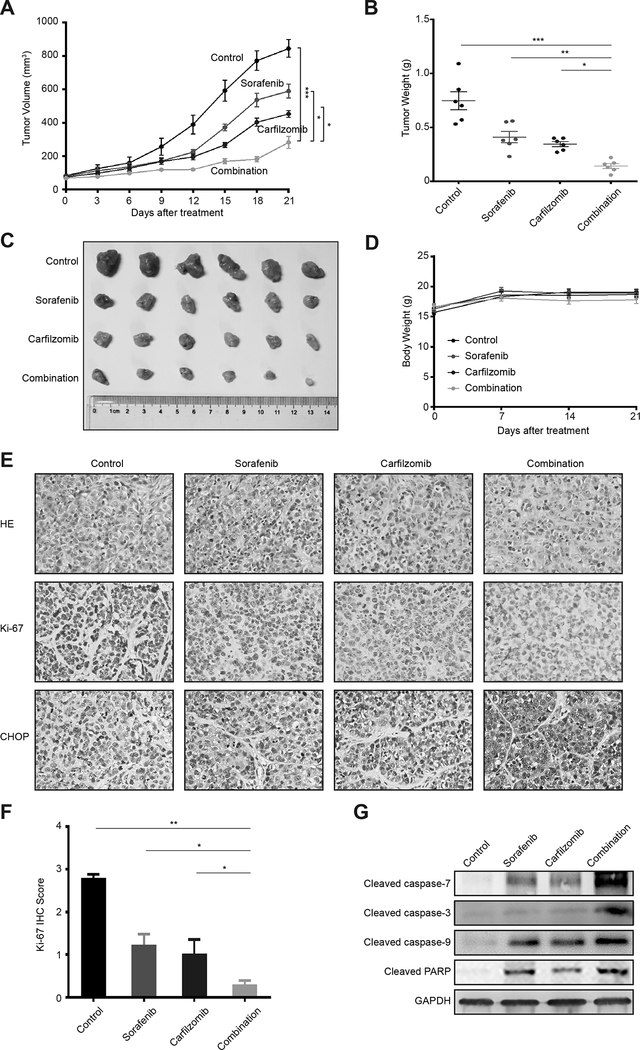
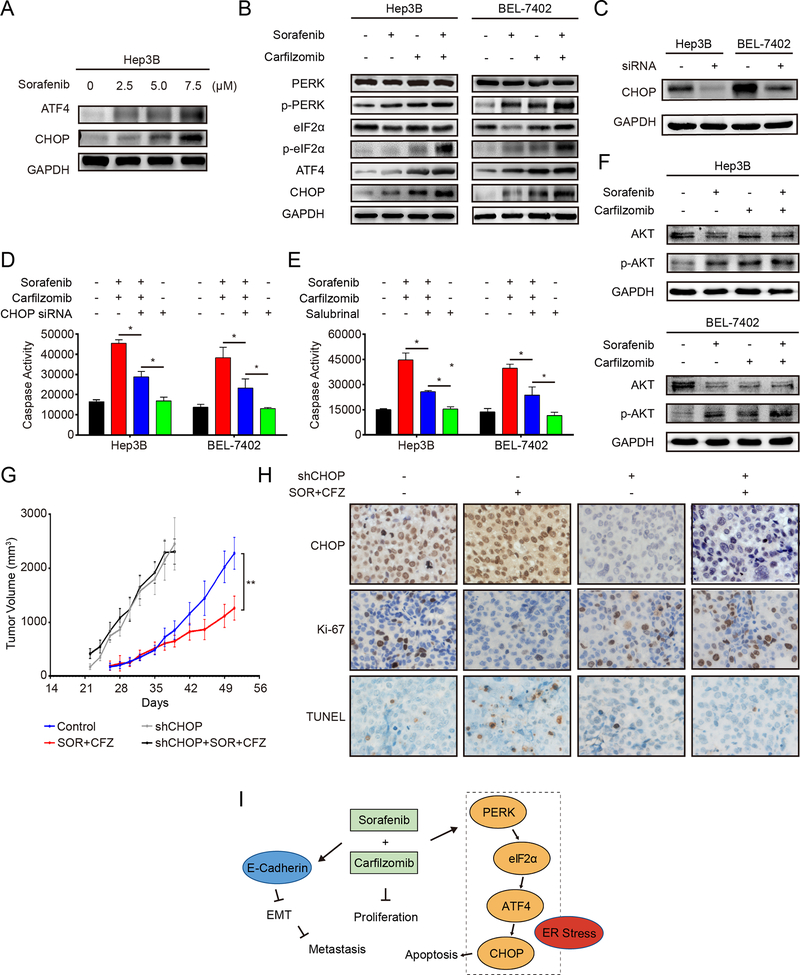
Hepatocellular carcinoma (HCC) is one of the most common and deadly human cancers. The 5-year survival rate is very low. Unfortunately, there are few efficacious therapeutic options. Until recently, Sorafenib has been the only available systemic drug for advanced HCC. However, it has very limited survival benefits, and new therapies are urgently needed. In this study, we investigated the anti-HCC activity of carfilzomib, a second-generation, irreversible proteasome inhibitor, as a single agent and in combination with sorafenib. In vitro, we found that carfilzomib has moderate anticancer activity toward liver cancer cells, but strongly enhances the ability of sorafenib to suppress HCC cell growth, proliferation, migration, invasion, and survival. Remarkably, the drug combination exhibits even more potent antitumor activity when tested in animal tumor models. Mechanistically, the combined treatment activates caspase-dependent and endoplasmic reticulum stress/CHOP-mediated apoptotic pathways, and suppresses epithelial-mesenchymal transition. In conclusion, our results demonstrate that the combination of carfilzomib and sorafenib has synergistic antitumor activities against HCC, providing a potential therapeutic strategy to improve the mortality and morbidity of HCC patients.
©2018 American Association for Cancer Research.
Conflict of interest statement
Conflicts of Interest
The authors declare no known conflicts of interest.
Figures
References
-
- Wilhelm SM, Carter C, Tang L, Wilkie D, McNabola A, Rong H, et al. BAY 43–9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer research 2004;64(19):7099–109 doi 10.1158/0008-5472.CAN-04-1443. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
