

Idelalisib promotes Bim-dependent apoptosis through AKT/FoxO3a in hepatocellular carcinoma
- PMID: 30224718
- PMCID: PMC6141589
- DOI: 10.1038/s41419-018-0960-8
Idelalisib promotes Bim-dependent apoptosis through AKT/FoxO3a in hepatocellular carcinoma
Retraction in
-
Retraction Note: Idelalisib promotes Bim-dependent apoptosis through AKT/FoxO3a in hepatocellular carcinoma.Cell Death Dis. 2024 Oct 24;15(10):773. doi: 10.1038/s41419-024-07162-y. Cell Death Dis. 2024. PMID: 39448559 Free PMC article. No abstract available.
Abstract
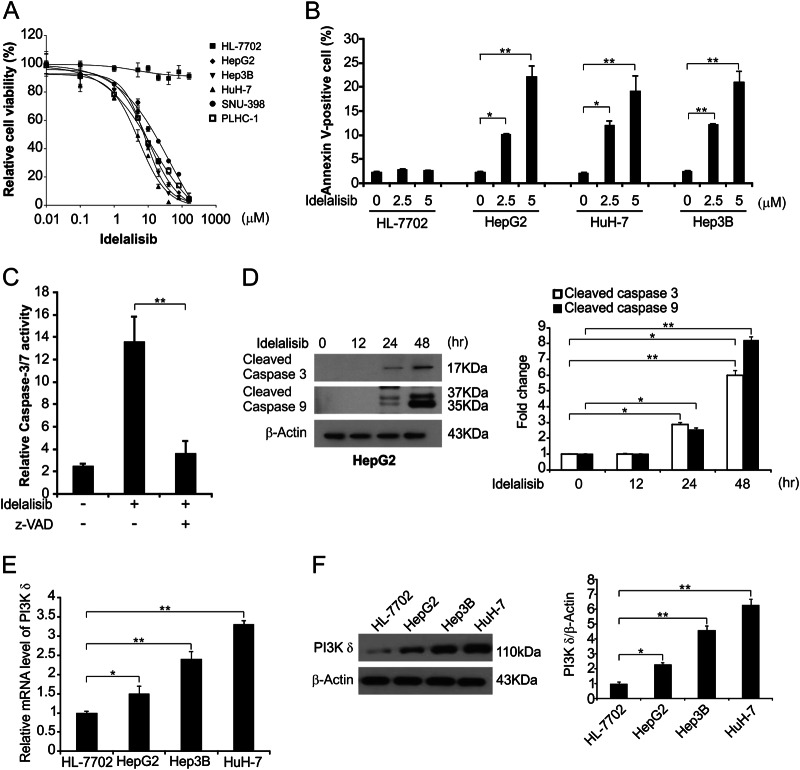
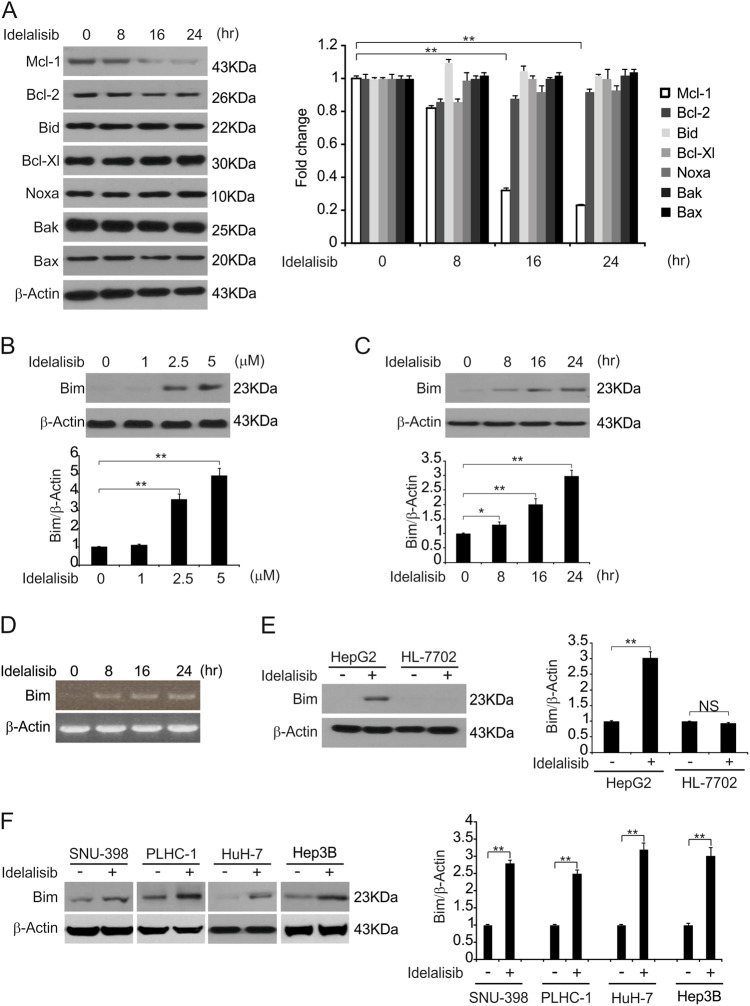
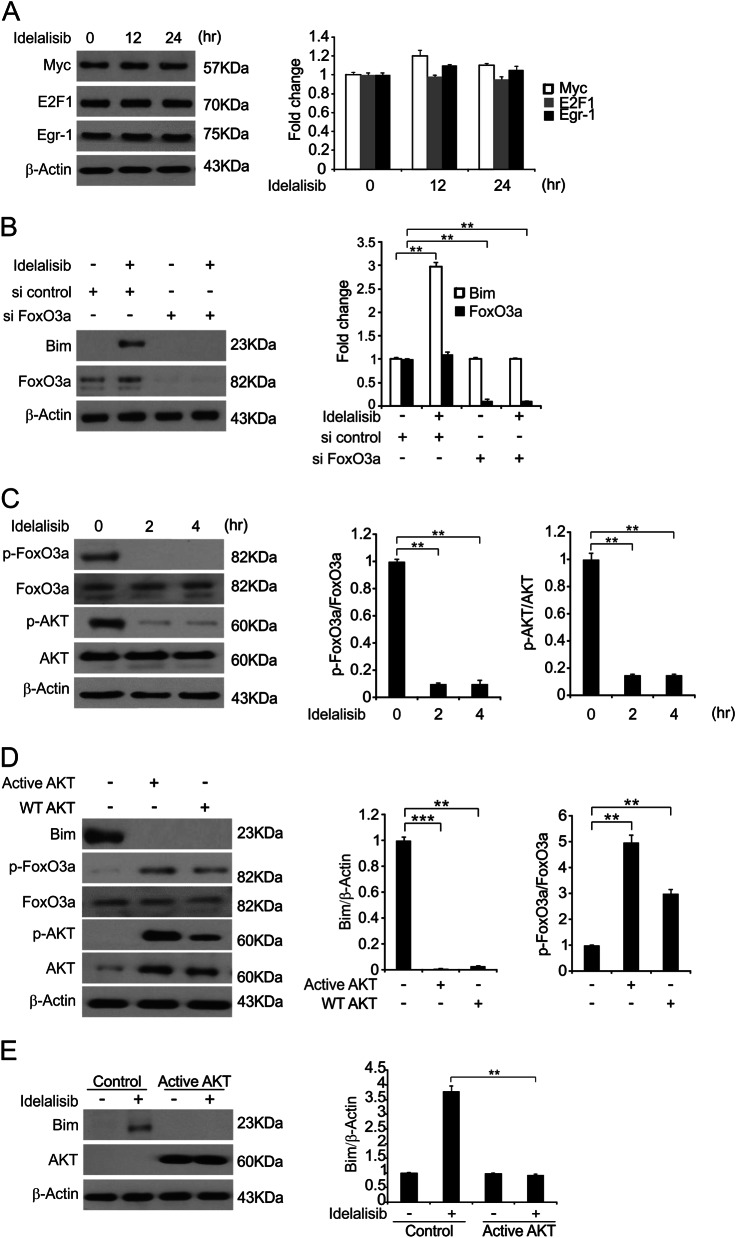
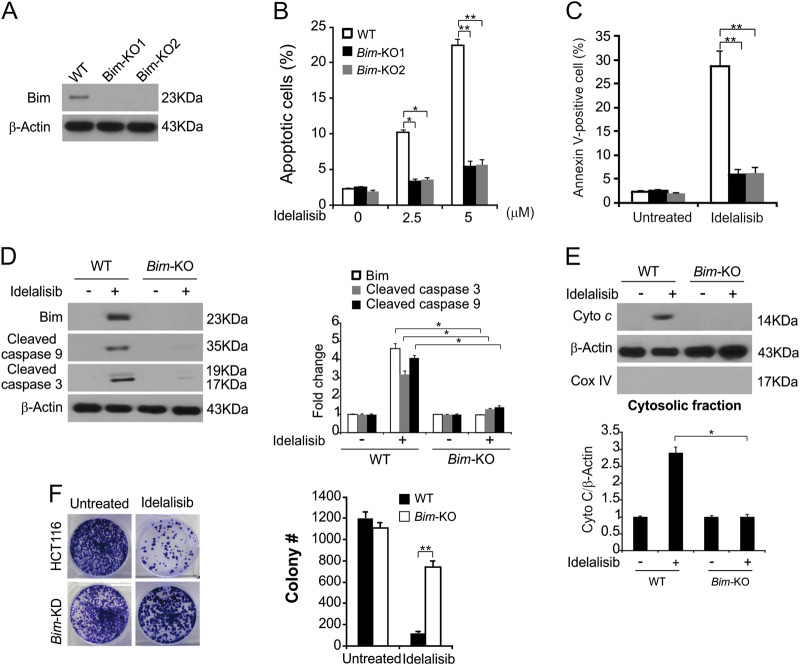
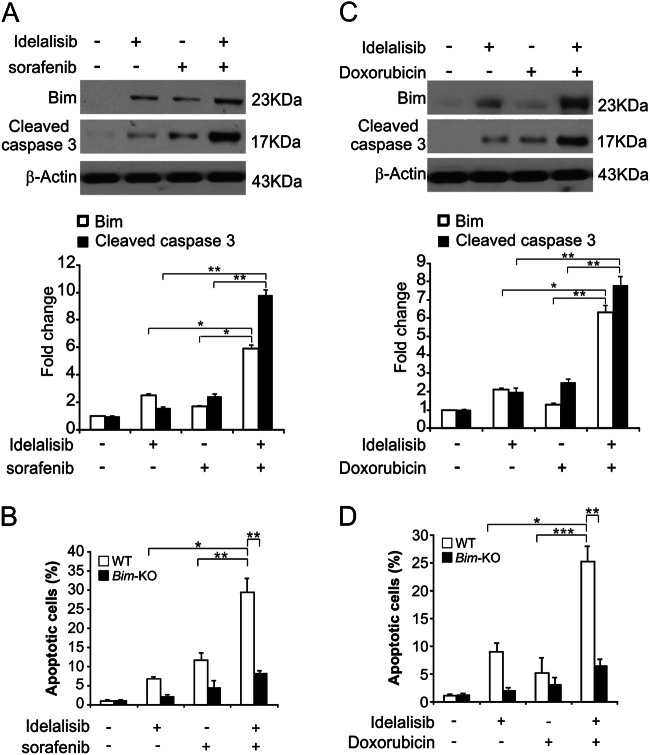
Idelalisib, a selective PI3Kδ inhibitor, has been approved by the FDA for chronic lymphocytic leukemia/small lymphocytic lymphoma treatment and for follicular lymphoma treatment when combined with rituximab. However, the mechanisms of effective action of idelalisib in hepatocellular carcinoma (HCC) remain unclear. In the current study, we aimed to investigate how idelalisib inhibits the growth of HCC cells and enhances the effects of other chemotherapeutic drugs. Our results show that idelalisib treatment promotes Bim induction in HCC via the FoxO3a pathway following PI3K/AKT inactivation. Moreover, our results show that Bim is required for idelalisib-mediated apoptosis in HCC. Idelalisib also synergizes with sorafenib or doxorubicin to induce significant apoptosis in HCC, and Bim is also necessary for the induction of apoptosis by cotreatment. Furthermore, a xenograft experiment reveals that the Bim deficiency abolishes apoptosis and antitumor effects of idelalisib in vivo. In summary, our results indicate a key role of Bim in mediating the antitumor effects of idelalisib in HCC. Our results also support the clinical significance of the drug.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
