

Serotonin receptor type 1B constitutes a therapeutic target for MDS and CMML
- PMID: 30224768
- PMCID: PMC6141614
- DOI: 10.1038/s41598-018-32306-4
Serotonin receptor type 1B constitutes a therapeutic target for MDS and CMML
Abstract
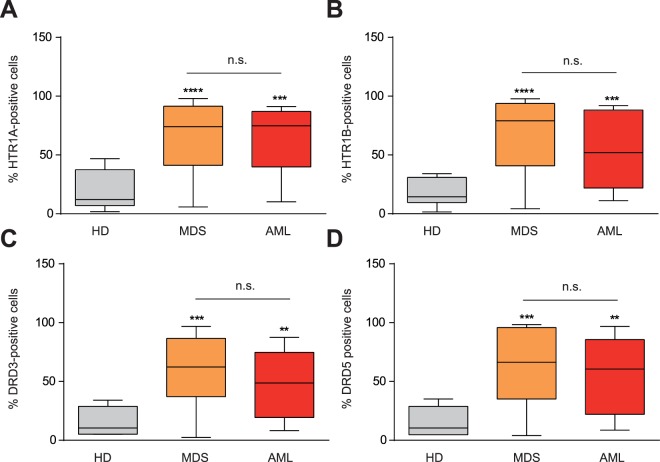
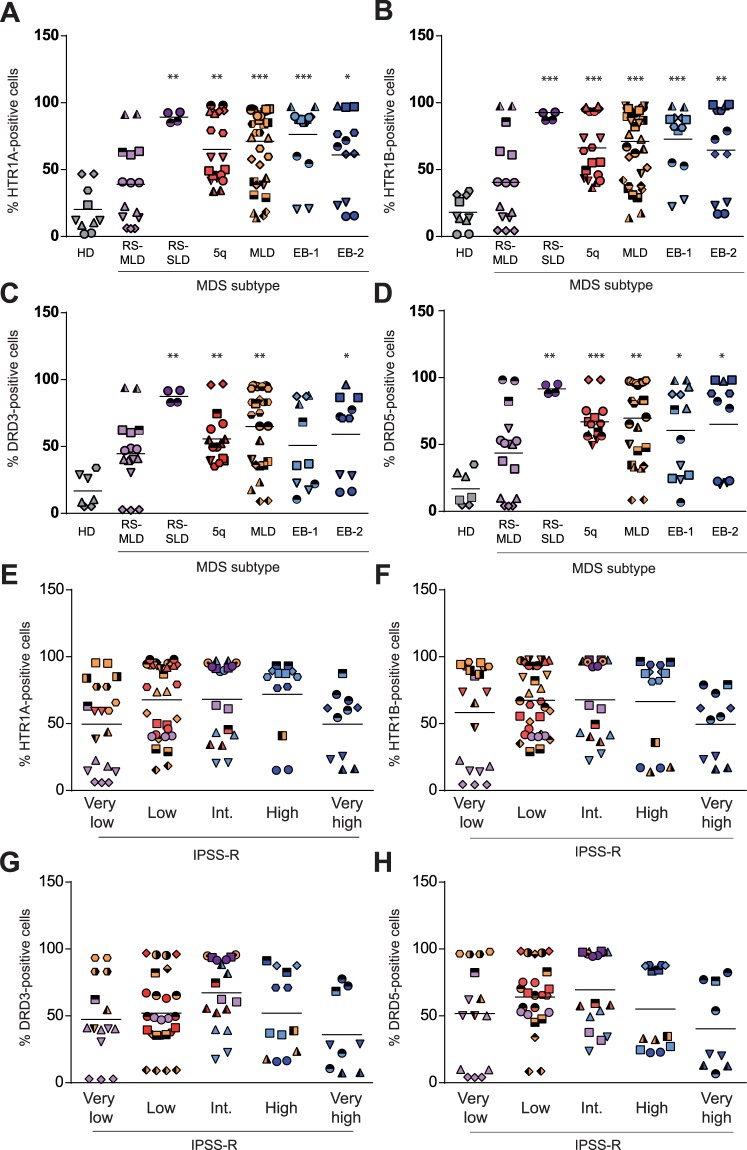
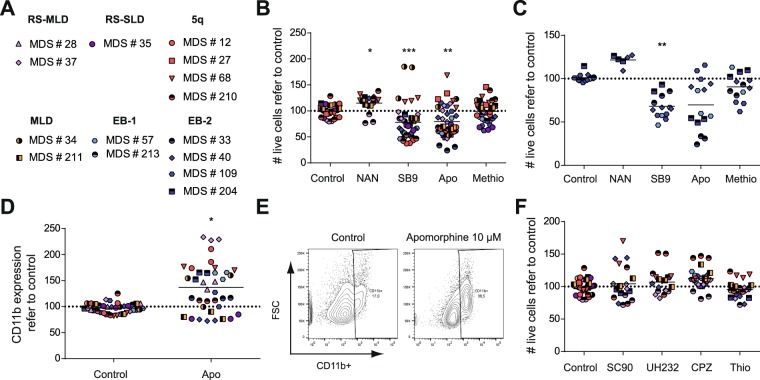
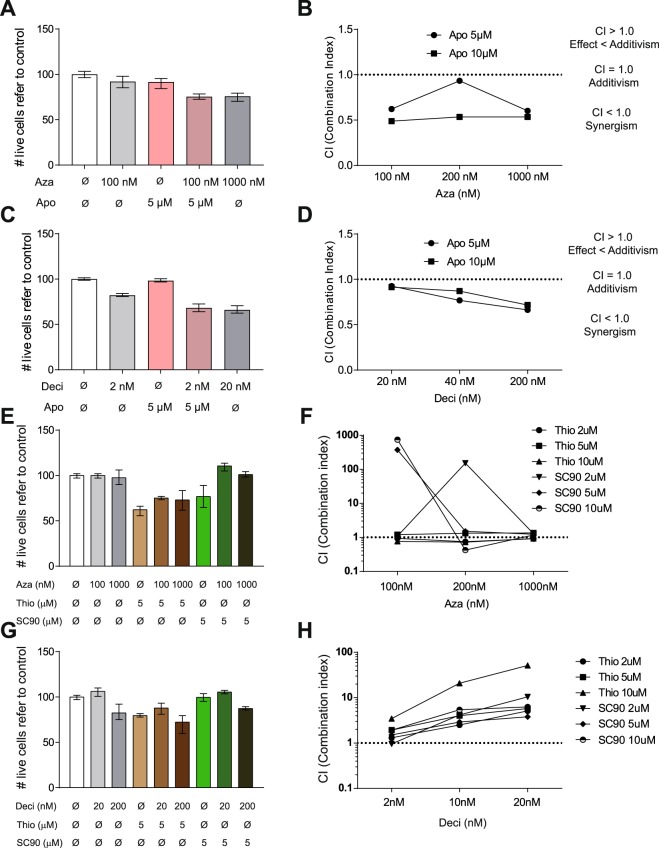
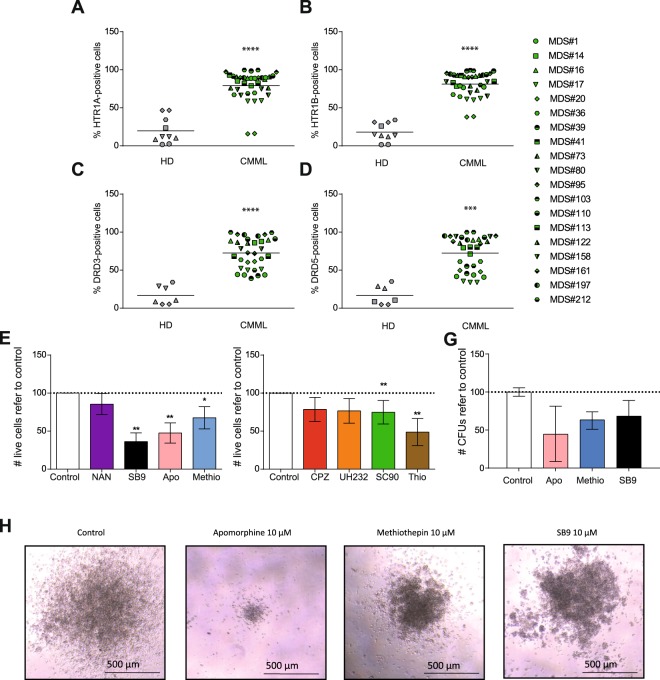
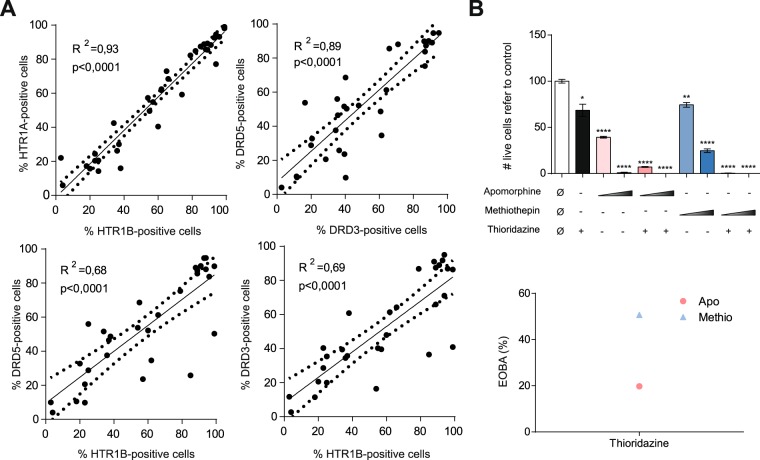
Myelodysplastic syndromes (MDS) and chronic myelomonocytic leukemia (CMML) are chronic myeloid clonal neoplasms. To date, the only potentially curative therapy for these disorders remains allogeneic hematopoietic progenitor cell transplantation (HCT), although patient eligibility is limited due to high morbimortality associated with this procedure coupled with advanced age of most patients. Dopamine receptors (DRs) and serotonin receptors type 1 (HTR1s) were identified as cancer stem cell therapeutic targets in acute myeloid leukemia. Given their close pathophysiologic relationship, expression of HTR1s and DRs was interrogated in MDS and CMML. Both receptors were differentially expressed in patient samples compared to healthy donors. Treatment with HTR1B antagonists reduced cell viability. HTR1 antagonists showed a synergistic cytotoxic effect with currently approved hypomethylating agents in AML cells. Our results suggest that HTR1B constitutes a novel therapeutic target for MDS and CMML. Due to its druggability, the clinical development of new regimens based on this target is promising.
Conflict of interest statement
The results presented in this paper have been patented. R.M.R. is a shareholder of Leukos Biotech.
Figures
References
-
- Beran M. Chronic myelomonocytic leukemia. Cancer Treat Res. 2008;142:107–132. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
